

Applications of the epidemiological modelling outputs for targeted mental health planning in conflict-affected populations: the Syria case-study
- PMID: 28596877
- PMCID: PMC5314753
- DOI: 10.1017/gmh.2016.4
Applications of the epidemiological modelling outputs for targeted mental health planning in conflict-affected populations: the Syria case-study
Abstract
Background: Epidemiological models are frequently utilised to ascertain disease prevalence in a population; however, these estimates can have wider practical applications for informing targeted scale-up and optimisation of mental health services. We explore potential applications for a conflict-affected population, Syria.
Methods: We use prevalence estimates of major depression and post-traumatic stress disorder (PTSD) in conflict-affected populations as inputs for subsequent estimations. We use Global Burden of Disease (GBD) methodology to estimate years lived with a disability (YLDs) for depression and PTSD in Syrian populations. Human resource (HR) requirements to scale-up recommended packages of care for PTSD and depression in Syria over a 15-year period were modelled using the World Health Organisation mhGAP costing tool. Associated avertable burden was estimated using health benefit analyses.
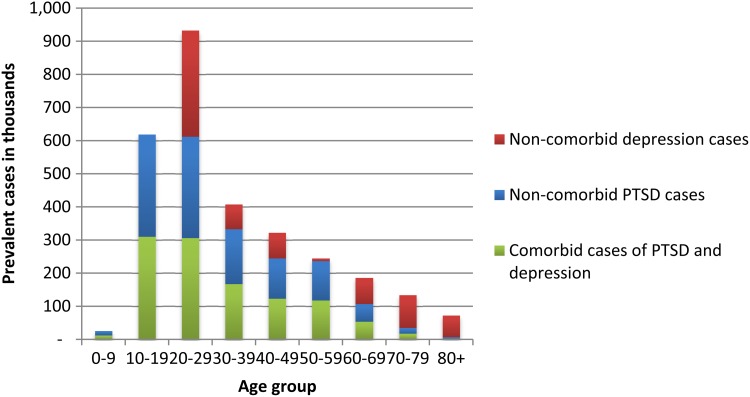
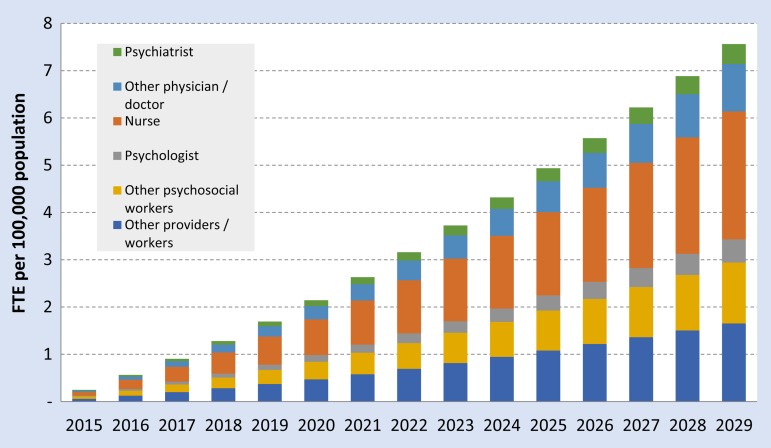
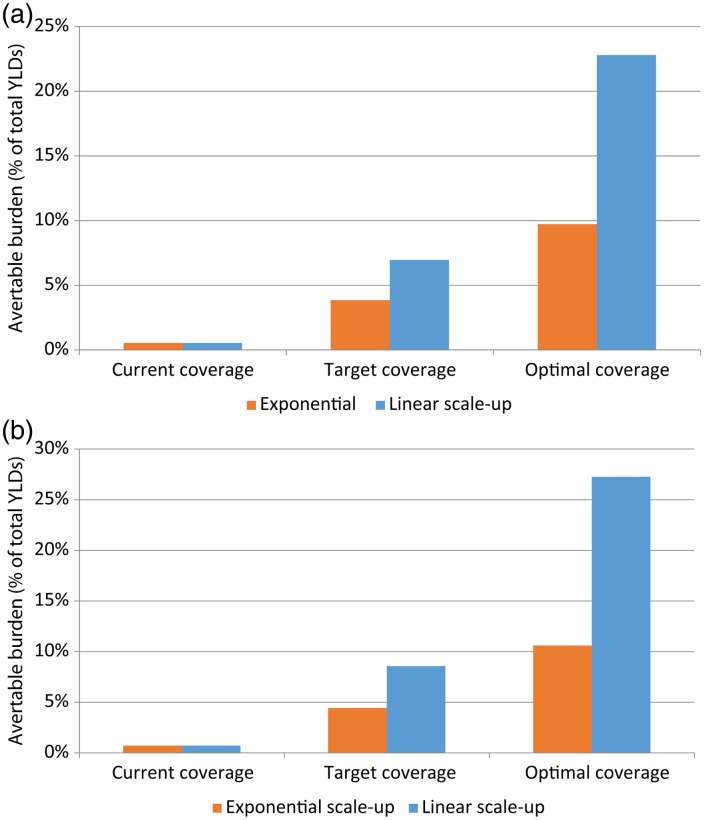
Results: The total number of cases of PTSD in Syria was estimated at approximately 2.2 million, and approximately 1.1 million for depression. An age-standardised major depression rate of 13.4 (95% UI 9.8-17.5) YLDs per 1000 Syrian population is estimated compared with the GBD 2010 global age-standardised YLD rate of 9.2 (95% UI 7.0-11.8). HR requirements to support a linear scale-up of services in Syria using the mhGAP costing tool demonstrates a steady increase from 0.3 FTE in at baseline to 7.6 FTE per 100 000 population after scale-up. Linear scale-up over 15 years could see 7-9% of disease burden being averted.
Conclusion: Epidemiological estimates of mental disorders are key inputs into determining disease burden and guiding optimal mental health service delivery and can be used in target populations such as conflict-affected populations.
Keywords: Conflict; depression; global mental health; policy & systems; post-traumatic stress disorder; service planning.
Figures

Similar articles
-
Post-traumatic stress disorder and major depression in conflict-affected populations: an epidemiological model and predictor analysis.Glob Ment Health (Camb). 2016 Feb 10;3:e4. doi: 10.1017/gmh.2015.26. eCollection 2016. Glob Ment Health (Camb). 2016. PMID: 28596873 Free PMC article.
-
New WHO prevalence estimates of mental disorders in conflict settings: a systematic review and meta-analysis.Lancet. 2019 Jul 20;394(10194):240-248. doi: 10.1016/S0140-6736(19)30934-1. Epub 2019 Jun 12. Lancet. 2019. PMID: 31200992 Free PMC article.
-
Prevalence of mental ill health, traumas and postmigration stress among refugees from Syria resettled in Sweden after 2011: a population-based survey.BMJ Open. 2017 Dec 29;7(12):e018899. doi: 10.1136/bmjopen-2017-018899. BMJ Open. 2017. PMID: 29289940 Free PMC article.
-
The global, regional, and national burden of inflammatory bowel disease in 195 countries and territories, 1990-2017: a systematic analysis for the Global Burden of Disease Study 2017.Lancet Gastroenterol Hepatol. 2020 Jan;5(1):17-30. doi: 10.1016/S2468-1253(19)30333-4. Epub 2019 Oct 21. Lancet Gastroenterol Hepatol. 2020. PMID: 31648971 Free PMC article.
-
A summary and appraisal of existing evidence of antimicrobial resistance in the Syrian conflict.Int J Infect Dis. 2018 Oct;75:26-33. doi: 10.1016/j.ijid.2018.06.010. Epub 2018 Jun 21. Int J Infect Dis. 2018. PMID: 29936319 Review.
Cited by
-
Conflict-related health research in Syria, 2011-2019: a scoping review for The Lancet - AUB Commission on Syria.Confl Health. 2021 Dec 14;15(1):92. doi: 10.1186/s13031-021-00384-3. Confl Health. 2021. PMID: 34906178 Free PMC article.
-
WHO mental health gap action programme (mhGAP) intervention guide: updated systematic review on evidence and impact.Evid Based Ment Health. 2021 Apr 26;24(3):124-30. doi: 10.1136/ebmental-2021-300254. Online ahead of print. Evid Based Ment Health. 2021. PMID: 33903119 Free PMC article. Review.
-
Psychological health problems among Syrians during war and the COVID-19 pandemic: national survey.BJPsych Int. 2021 Aug;18(3):E8. doi: 10.1192/bji.2021.16. BJPsych Int. 2021. PMID: 34382955 Free PMC article. Review.
-
Is only one cognitive technique also effective? Results from a randomized controlled trial of two different versions of an internet-based cognitive behavioural intervention for post-traumatic stress disorder in Arabic-speaking countries.Eur J Psychotraumatol. 2021 Jul 15;12(1):1943870. doi: 10.1080/20008198.2021.1943870. eCollection 2021. Eur J Psychotraumatol. 2021. PMID: 34345377 Free PMC article. Clinical Trial.
-
Refugee Mental Health, Global Health Policy, and the Syrian Crisis.Front Public Health. 2021 Aug 3;9:676000. doi: 10.3389/fpubh.2021.676000. eCollection 2021. Front Public Health. 2021. PMID: 34414156 Free PMC article.
References
-
- American Psychiatric Association (2000). Diagnostic and Statistical Manual of Mental Disorders (DSM-IV-TR). American Psychiatric Association: Washington, DC.
-
- Andrews G, Sanderson K, Corry J, Lapsley HM (2000). Using epidemiological data to model efficiency in reducing the burden of depression. Journal of Mental Health Policy and Economics 3, 175–186. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources