

Recurrent Post-Ablation Paroxysmal Atrial Fibrillation Shares Substrates With Persistent Atrial Fibrillation : An 11-Center Study
- PMID: 28596994
- PMCID: PMC5458418
- DOI: 10.1016/j.jacep.2016.10.006
Recurrent Post-Ablation Paroxysmal Atrial Fibrillation Shares Substrates With Persistent Atrial Fibrillation : An 11-Center Study
Abstract
Introduction: The role of atrial fibrillation (AF) substrates is unclear in patients with paroxysmal AF (PAF) that recurs after pulmonary vein isolation (PVI). We hypothesized that patients with recurrent post-ablation (redo) PAF despite PVI have electrical substrates marked by rotors and focal sources, and structural substrates that resemble persistent AF more than patients with (de novo) PAF at first ablation.
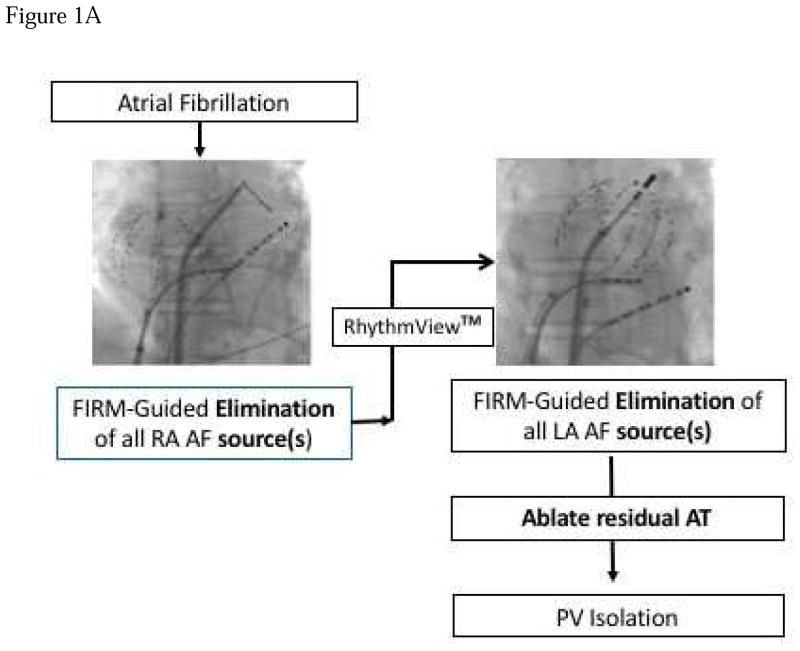
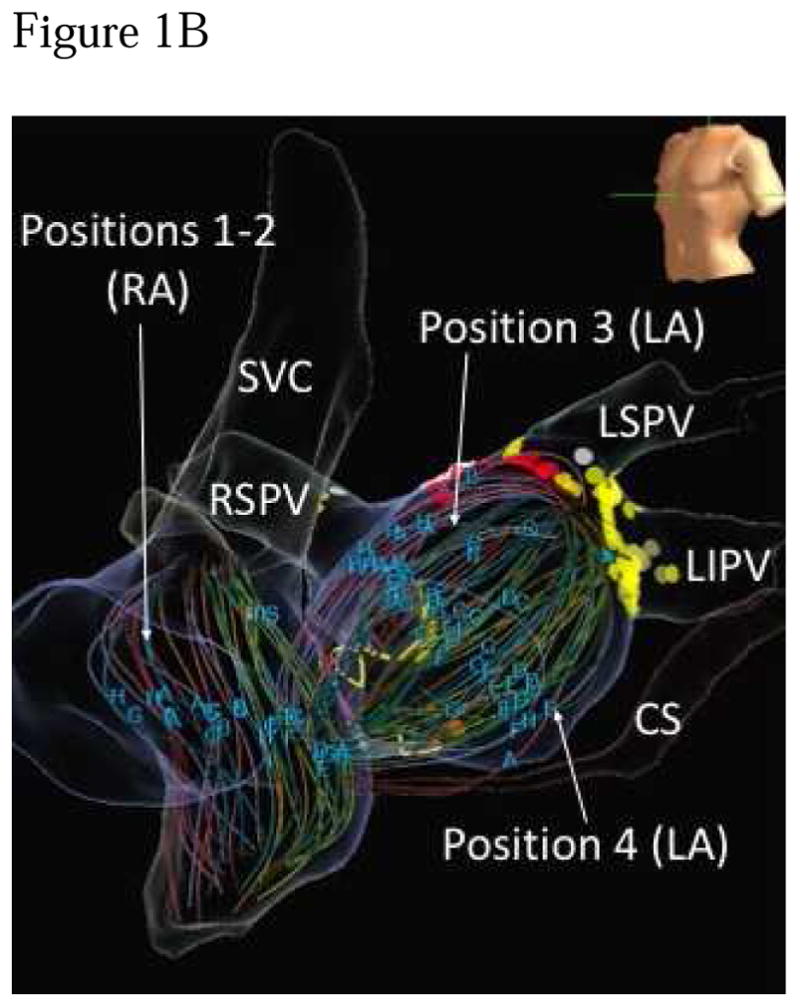
Methods: In 175 patients at 11 centers, we compared AF substrates in both atria using 64 pole-basket catheters and phase mapping, and indices of anatomical remodeling between patients with de novo or redo PAF and first ablation for persistent AF.
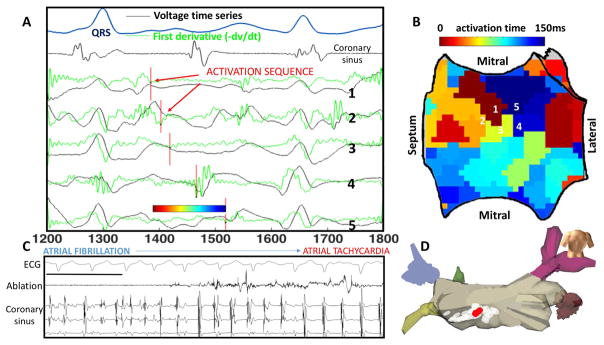
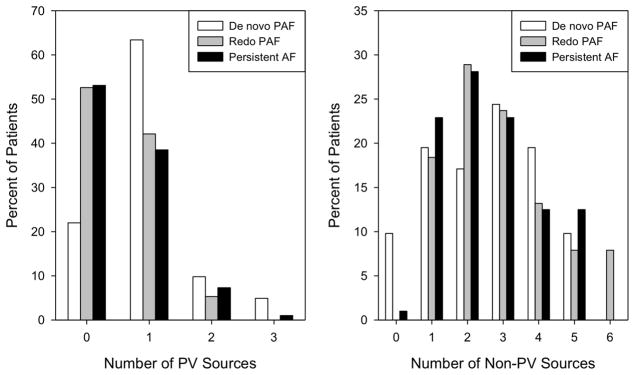
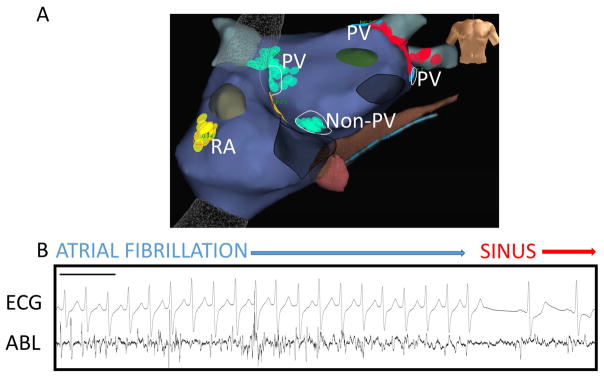
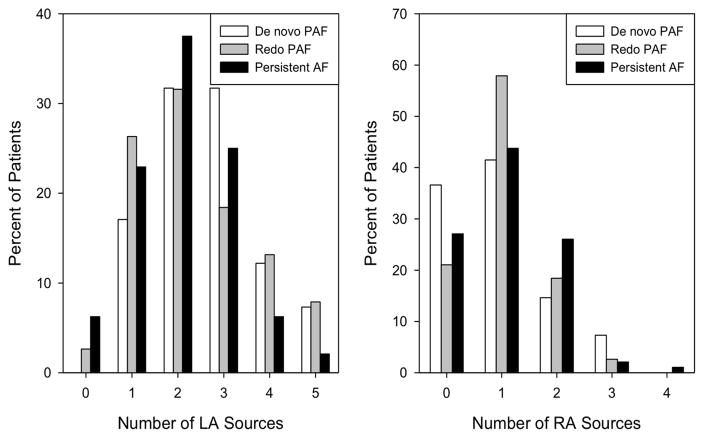
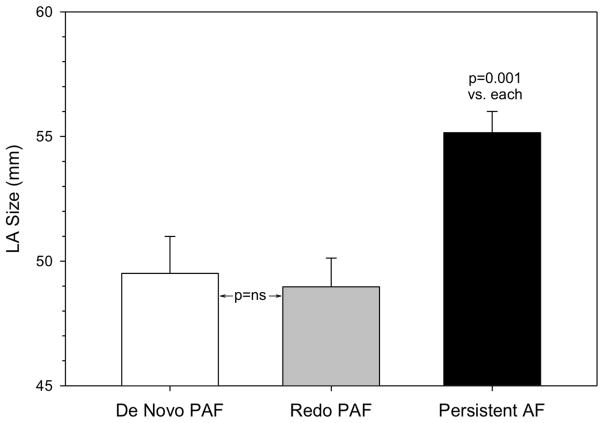
Results: Sources were seen in all patients. More patients with de novo PAF (78.0%) had sources near PVs than patients with redo PAF (47.4%, p=0.005) or persistent AF (46.9%, p=0.001). The total number of sources per patient (p=0.444), and number of non-PV sources (p=0.701) were similar between groups, indicating that redo PAF patients had residual non-PV sources after elimination of PV sources by prior PVI. Structurally, left atrial size did not separate de novo from redo PAF (49.5±9.5 vs. 49.0±7.1mm, p=0.956) but was larger in patients with persistent AF (55.2±8.4mm, p=0.001).
Conclusions: Patients with paroxysmal AF despite prior PVI show electrical substrates that resemble persistent AF more closely than patients with paroxysmal AF at first ablation. Notably, these subgroups of paroxysmal AF are indistinguishable by structural indices. These data motivate studies of trigger versus substrate mechanisms for patients with recurrent paroxysmal AF after PVI.
Keywords: ablation; atrial fibrillation; sources.
Figures
Comment in
-
The Dynamic Substrate for Atrial Fibrillation: Can We Identify It and Is It of Clinical Importance?JACC Clin Electrophysiol. 2017 Apr;3(4):403-404. doi: 10.1016/j.jacep.2016.12.003. Epub 2017 Feb 1. JACC Clin Electrophysiol. 2017. PMID: 29759453 No abstract available.
-
Are Rotors Markers of Substrate or a Mechanism of Perpetuation of Atrial Fibrillation?: Rotor Ablation in AF: Many Unanswered Questions.JACC Clin Electrophysiol. 2017 Nov;3(11):1339-1340. doi: 10.1016/j.jacep.2017.07.020. Epub 2017 Nov 20. JACC Clin Electrophysiol. 2017. PMID: 29759636 No abstract available.
-
Reply: Are Rotors Markers of Substrate or a Mechanism of Perpetuation of Atrial Fibrillation? Increasing Data for Rotational Drivers of Human AF.JACC Clin Electrophysiol. 2017 Nov;3(11):1340-1341. doi: 10.1016/j.jacep.2017.08.015. Epub 2017 Nov 20. JACC Clin Electrophysiol. 2017. PMID: 29759637 No abstract available.
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials