

Improved pregnancy outcomes in women with type 1 and type 2 diabetes but substantial clinic-to-clinic variations: a prospective nationwide study
- PMID: 28597075
- PMCID: PMC5552835
- DOI: 10.1007/s00125-017-4314-3
Improved pregnancy outcomes in women with type 1 and type 2 diabetes but substantial clinic-to-clinic variations: a prospective nationwide study
Abstract
Aims/hypothesis: The aim of this prospective nationwide study was to examine antenatal pregnancy care and pregnancy outcomes in women with type 1 and type 2 diabetes, and to describe changes since 2002/2003.
Methods: This national population-based cohort included 3036 pregnant women with diabetes from 155 maternity clinics in England and Wales who delivered during 2015. The main outcome measures were maternal glycaemic control, preterm delivery (before 37 weeks), infant large for gestational age (LGA), and rates of congenital anomaly, stillbirth and neonatal death.
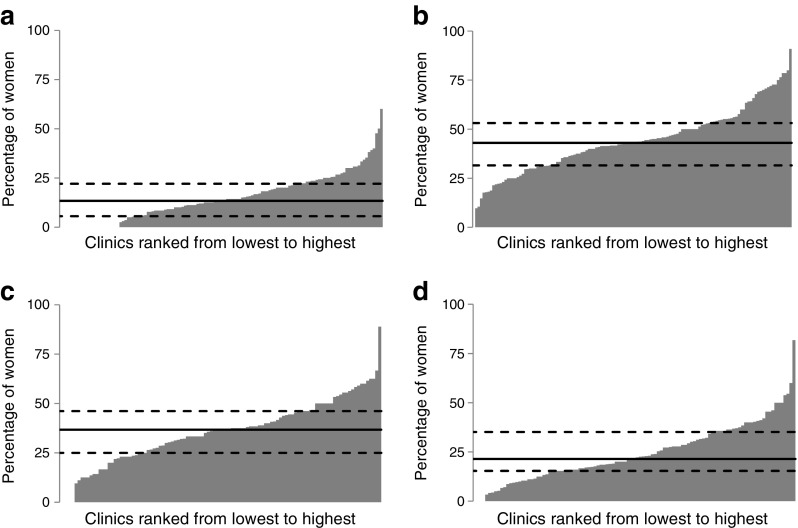
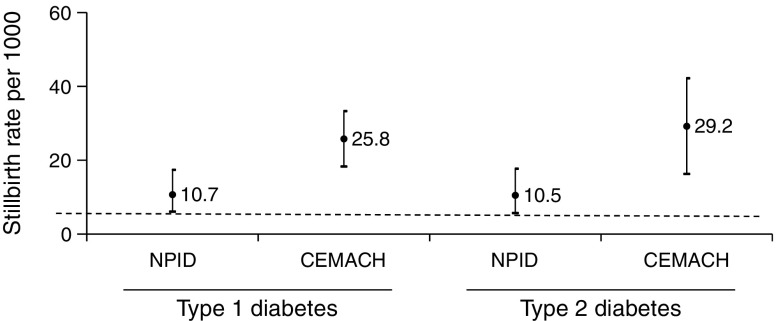
Results: Of 3036 women, 1563 (51%) had type 1, 1386 (46%) had type 2 and 87 (3%) had other types of diabetes. The percentage of women achieving HbA1c < 6.5% (48 mmol/mol) in early pregnancy varied greatly between clinics (median [interquartile range] 14.3% [7.7-22.2] for type 1, 37.0% [27.3-46.2] for type 2). The number of infants born preterm (21.7% vs 39.7%) and LGA (23.9% vs 46.4%) were lower for women with type 2 compared with type 1 diabetes (both p < 0.001). The prevalence rates for congenital anomaly (46.2/1000 births for type 1, 34.6/1000 births for type 2) and neonatal death (8.1/1000 births for type 1, 11.4/1000 births for type 2) were unchanged since 2002/2003. Stillbirth rates are almost 2.5 times lower than in 2002/2003 (10.7 vs 25.8/1000 births for type 1, p = 0.0012; 10.5 vs 29.2/1000 births for type 2, p = 0.0091).
Conclusions/interpretation: Stillbirth rates among women with type 1 and type 2 diabetes have decreased since 2002/2003. Rates of preterm delivery and LGA infants are lower in women with type 2 compared with type 1 diabetes. In women with type 1 diabetes, suboptimal glucose control and high rates of perinatal morbidity persist with substantial variations between clinics.
Data availability: Further details of the data collection methodology, individual clinic data and the full audit reports for healthcare professionals and service users are available from http://content.digital.nhs.uk/npid .
Keywords: Antenatal; Congenital anomaly; Diabetes; Glucose; Large for gestational age; Neonatal; Pre-pregnancy care; Pregnancy; Preterm; Stillbirth.
Conflict of interest statement
Data availability
Further details of the data collection methodology, individual clinic data and the full audit reports for healthcare professionals and service users are available from
Funding
The NPID audit is commissioned by the Healthcare Quality Improvement Partnership as part of the National Clinical Audit programme funded by NHS England and the Welsh government. The 2015 audit was prepared in collaboration with NHS Digital and supported by Diabetes UK and Public Health England.
Duality of interest
HRM sits on a scientific advisory board for Medtronic (insulin pump manufacturer). The authors declare that there is no duality of interest associated with this manuscript.
Contribution statement
HRM, RB, MMa, MMo, NLB, BY made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data. CC, PC and CS analysed the data. HRM drafted the manuscript. All authors critically reviewed the manuscript for important intellectual content and gave final approval for publication. HRM is the guarantor of this work.
Figures
References
-
- Evers IM, de Valk HW, Visser GH. Risk of complications of pregnancy in women with type 1 diabetes: nationwide prospective study in the Netherlands. BMJ. 2004;328:915. doi: 10.1136/bmj.38043.583160.EE. - DOI - PMC - PubMed
-
- Macintosh MC, Fleming KM, Bailey JA, et al. Perinatal mortality and congenital anomalies in babies of women with type 1 or type 2 diabetes in England, Wales, and Northern Ireland: population based study. BMJ. 2006;333:177. doi: 10.1136/bmj.38856.692986.AE. - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
