

Pharmacokinetic Profile of a 2-Month Dose Regimen of Aripiprazole Lauroxil: A Phase I Study and a Population Pharmacokinetic Model
- PMID: 28597226
- PMCID: PMC5511303
- DOI: 10.1007/s40263-017-0447-7
Pharmacokinetic Profile of a 2-Month Dose Regimen of Aripiprazole Lauroxil: A Phase I Study and a Population Pharmacokinetic Model
Abstract
Background: Aripiprazole lauroxil (AL) is a long-acting injectable medication approved for the treatment of schizophrenia. Current AL regimens are 441 mg, 662 mg, and 882 mg administered monthly (every 4 weeks [q4wk]), or 882 mg administered every 6 weeks (q6wk).
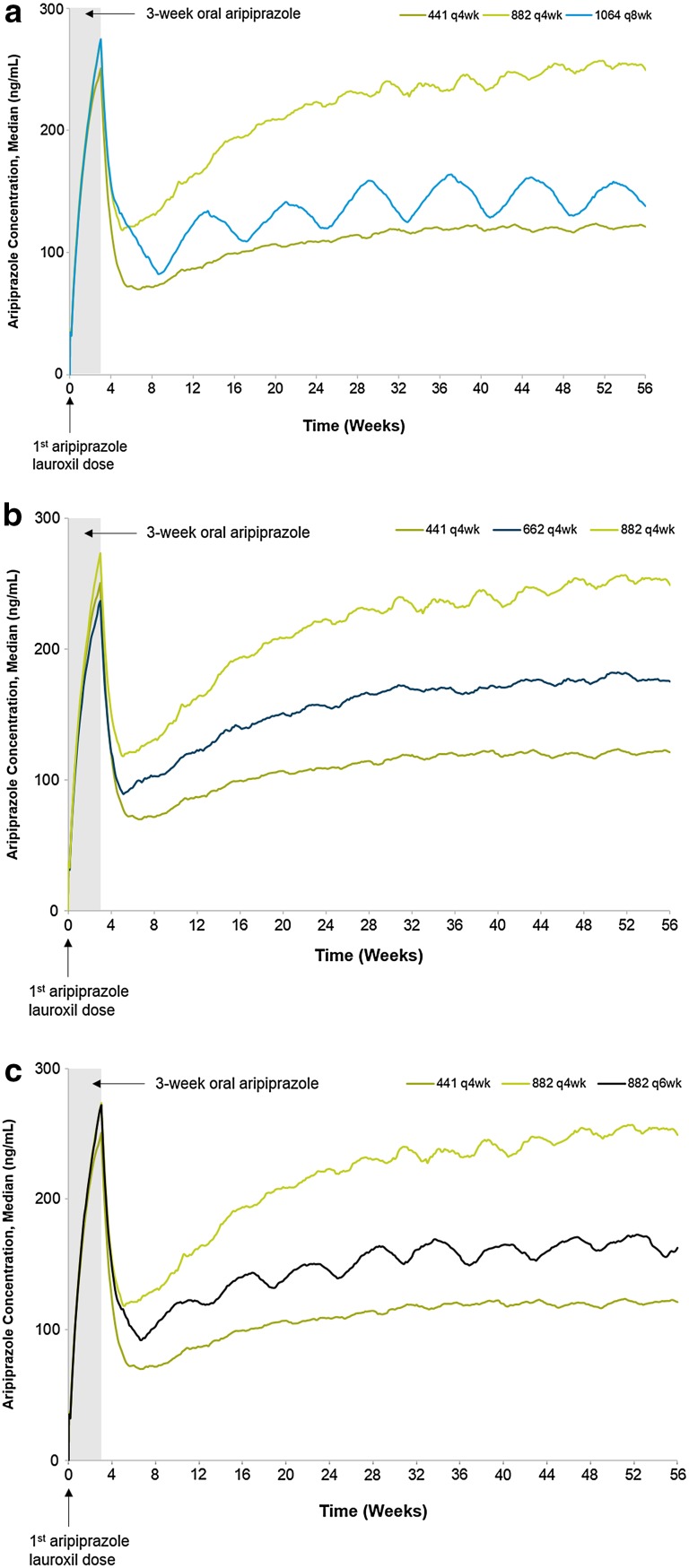
Objective: We examined the feasibility of a 2-month (every 8 weeks [q8wk]) dosing interval of AL in a phase I open-label pharmacokinetic study investigating AL 1064 mg administered q8wk for 24 weeks, followed by 20 weeks of safety and pharmacokinetic measurements (ClinicalTrials.gov ID: NCT02320032). Second, a population pharmacokinetic model (referred to as the 2MPopPK model) was generated using data collected from the present trial, as well as data obtained from earlier studies.
Methods: The phase I study included patients with schizophrenia or schizoaffective disorder maintained on an oral antipsychotic (n = 140) who were assigned to one of three groups: AL 441 mg q4wk, AL 882 mg q6wk, or AL 1064 mg q8wk, with a total of seven, five, or four injections administered, respectively. No oral aripiprazole lead-in supplementation was administered and patients continued on maintenance oral antipsychotics. Pharmacokinetic samples were collected at various time points during the 24-week study period and the 20-week follow-up period. Plasma concentrations obtained from the phase I study were analyzed using non-compartmental methods. Additionally, the data were combined with data collected from prior studies to develop the 2MPopPK model.
Results: Following the final injection of AL in the phase I study, maximum aripiprazole concentrations were achieved 24.4-35.2 days after the last dose and persisted for the duration of the study. The mean C avg,ss values were 125.8 ng/ml, 131.1 ng/ml, and 140.7 ng/ml for the 441 mg q4wk, 882 mg q6wk, and 1064 mg q8wk doses, respectively. The mean elimination half-life of aripiprazole following the last dose was 53.9 days for the 1064 mg dose, 55.1 days for the 882 mg dose, and 57.2 days for the 441 mg dose. The 2MPopPK dataset included 14,524 aripiprazole concentrations from 700 patients with schizophrenia. The duration of absorption of aripiprazole was estimated as 43 days (95% confidence interval [CI] 42-45 days), which was preceded by a 3.2-day lag time (95% CI 3.0-3.5 days) for a total duration of input into the systemic circulation of 46 days following intramuscular administration of AL. Multiple-dose simulations showed that the 1064 mg q8wk regimen provides aripiprazole concentrations within the concentration range associated with 441 mg and 882 mg q4wk doses previously demonstrated to be efficacious in a phase III study.
Conclusion: These data from the phase I study and the 2MPopPK model support the suitability of using the AL 1064 mg dose as a 2-month (q8wk) dose interval option for the treatment of schizophrenia.
Conflict of interest statement
Conflicts of interest
Dr Hard is a former employee of Alkermes and is presently an employee of Nuventra Pharma Sciences. Drs Wehr, Weiden, and von Moltke are employees of Alkermes. Drs Sadler and Mills are employees of ICON plc and contracted by Alkermes to perform the work described in this manuscript.
Funding
This study was sponsored by Alkermes Inc.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Figures


References
-
- Lindenmayer JP, Liu-Seifert H, Kulkarni PM, Kinon BJ, Stauffer V, Edwards SE, et al. Medication nonadherence and treatment outcome in patients with schizophrenia or schizoaffective disorder with suboptimal prior response. J Clin Psychiatry. 2009;70(7):990–996. doi: 10.4088/JCP.08m04221. - DOI - PubMed
-
- Alkermes Inc. Aristada (Aripiprazole Lauroxil) Prescribing Information. 2017. https://www.aristadahcp.com/downloadables/ARISTADA-PI.pdf. Accessed May 2017.
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
