

Lesinurad, a Selective Uric Acid Reabsorption Inhibitor, in Combination With Febuxostat in Patients With Tophaceous Gout: Findings of a Phase III Clinical Trial
- PMID: 28597604
- PMCID: PMC5601200
- DOI: 10.1002/art.40159
Lesinurad, a Selective Uric Acid Reabsorption Inhibitor, in Combination With Febuxostat in Patients With Tophaceous Gout: Findings of a Phase III Clinical Trial
Abstract
Objective: To investigate the efficacy and safety of lesinurad in combination with febuxostat in a 12-month phase III trial in patients with tophaceous gout.
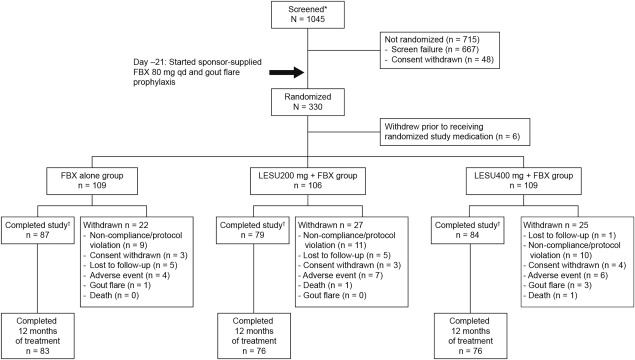
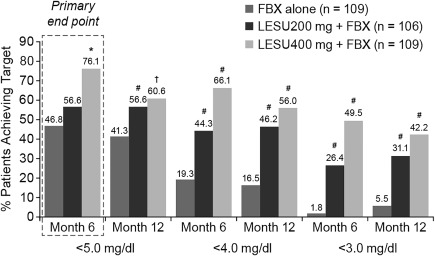
Methods: Patients with serum urate (UA) ≥8.0 mg/dl (≥6.0 mg/dl with urate-lowering therapy) and ≥1 measurable target tophus were given febuxostat 80 mg/day for 3 weeks before randomization to receive lesinurad (200 or 400 mg daily) or placebo in addition to the febuxostat. The primary end point was the proportion of patients achieving a serum UA level of <5.0 mg/dl (month 6). The key secondary end point was the proportion of patients with complete resolution of ≥1 target tophus (month 12). Other end points included the percentage change in total target tophi area. Safety assessments included adverse events and laboratory data.
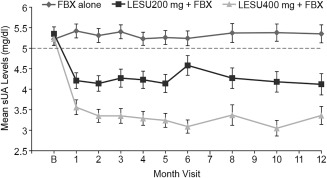
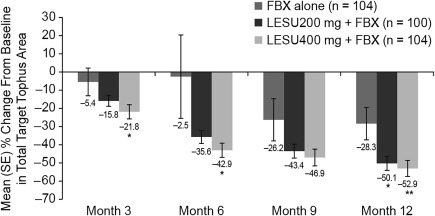
Results: Patients (n = 324) were predominantly male, with a mean age of 54.1 years. Significantly more patients achieved the serum UA target by month 6 with the addition of lesinurad 400 mg (76.1%; P < 0.0001), but not 200 mg (56.6%; P = 0.13), to the febuxostat therapy as compared with febuxostat alone (46.8%). At all other time points, significantly more patients in the lesinurad 200 mg group achieved the serum UA target. The number of patients with complete tophus resolution was not different between groups. Treatment with lesinurad (200 mg and 400 mg) plus febuxostat reduced the total target tophi area as compared with febuxostat alone (50.1% and 52.9% versus 28.3%, respectively; P < 0.05). Safety was generally comparable with that of febuxostat alone, except for higher rates of predominantly reversible elevations in the serum creatinine level, particularly with lesinurad 400 mg.
Conclusion: Treatment with lesinurad in combination with febuxostat demonstrated superior lowering of serum UA levels as compared with febuxostat alone, with clinically relevant added effects on tophi and an acceptable safety profile with lesinurad 200 mg in patients with tophaceous gout warranting additional therapy.
Trial registration: ClinicalTrials.gov NCT01510769.
© 2017 The Authors. Arthritis & Rheumatology published by Wiley Periodicals, Inc. on behalf of American College of Rheumatology.
Figures
References
-
- Richette P, Doherty M, Pascual E, Barskova V, Becce F, Castaneda‐Sanabria J, et al. 2016 updated EULAR evidence‐based recommendations for the management of gout. Ann Rheum Dis 2017;76:29–42. - PubMed
-
- Kiltz U, Smolen J, Bardin T, Cohen SA, Dalbeth N, Doherty M, et al. Treat‐to‐target (T2T) recommendations for gout. Ann Rheum Dis 2016;76:632–8. - PubMed
-
- Becker MA, Schumacher HR Jr, Wortmann RL, MacDonald PA, Eustace D, Palo WA, et al. Febuxostat compared with allopurinol in patients with hyperuricemia and gout. N Engl J Med 2005;353:2450–61. - PubMed
