

A systematic review of transition studies of pulmonary arterial hypertension specific medications
- PMID: 28597769
- PMCID: PMC5467943
- DOI: 10.1177/2045893217706357
A systematic review of transition studies of pulmonary arterial hypertension specific medications
Abstract
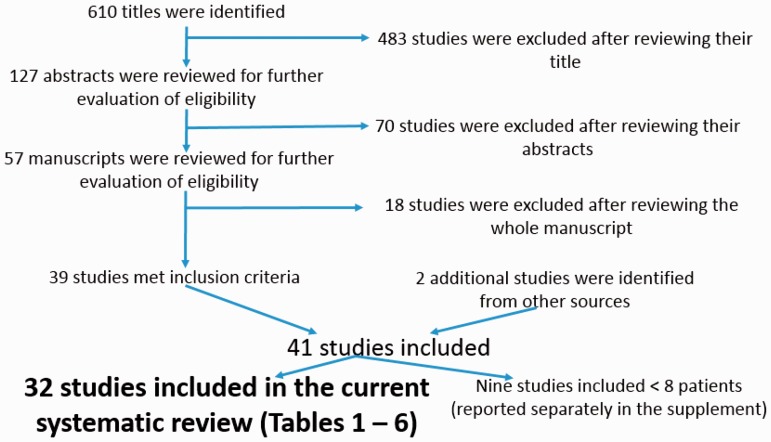
Pulmonary arterial hypertension (PAH) is a progressive potentially fatal disease. Multiple pharmacologic options are now available, which facilitated transitions between different therapeutic options, although the evidence for such transitions has not been well described. We sought to review the evidence supporting the safety and/or efficacy of transitioning between PAH-specific medications. We performed a systematic review of all published studies in the Medline database between 1 January 2000 and 30 June 2016 reporting on any transition between the currently Food and Drug Administration (FDA)-approved PAH-specific medications. Studies reporting on three or more adult patients published in the English language reporting on transitions between FDA-approved PAH medications were extracted and tabulated. Forty-one studies met the selection criteria, nine of which included less than eight patients (and thus were reported separately in the supplement), for a total of 32 studies. Transitioning from parenteral epoprostenol to parenteral treprostinil appears to be safe and efficacious in patients who have less severe disease and more favorable hemodynamics. Transitioning from a prostacyclin analogue to an oral medication may be successful in patients who have favorable hemodynamics and stable disease. There is conflicting evidence supporting the transition from a parenteral to an inhaled prostacyclin analogue, even in patients who are on background oral therapy. Currently, the only evidence in support of transitioning between oral PDE5 inhibitors is from sildenafil to tadalafil. Patients on higher doses of sildenafil are more likely to fail. In patients with liver abnormalities due to bosentan or sitaxentan, the transition to ambrisentan appears to be safe and can result in clinical improvement. Studies regarding PAH medication transitions are limited. Patients who have less severe disease, better functional status, and are on lower medications doses may be more successful at transitioning.
Keywords: pharmacotherapy; pulmonary arterial hypertension; pulmonary hypertension; pulmonary vascular disease; transition.
Figures
References
-
- Benza RL, Gomberg-Maitland M, Miller DP, et al. The REVEAL Registry risk score calculator in patients newly diagnosed with pulmonary arterial hypertension. Chest 2012; 141(2): 354–362. - PubMed
-
- D’Alonzo GE, Barst RJ, Ayres SM, et al. Survival in patients with primary pulmonary hypertension. Results from a national prospective registry. Ann Intern Med 1991; 115(5): 343–349. - PubMed
-
- McGoon MD, Benza RL, Escribano-Subias P, et al. Pulmonary arterial hypertension: epidemiology and registries. J Am Coll Cardiol 2013; 62(25 Suppl): D51–59. - PubMed
-
- Galie N, Humbert M, Vachiery JL, et al. 2015 ESC/ERS Guidelines for the diagnosis and treatment of pulmonary hypertension: The Joint Task Force for the Diagnosis and Treatment of Pulmonary Hypertension of the European Society of Cardiology (ESC) and the European Respiratory Society (ERS): Endorsed by: Association for European Paediatric and Congenital Cardiology (AEPC), International Society for Heart and Lung Transplantation (ISHLT). Eur Respir J 2015; 46(4): 903–975. - PubMed
-
- Galie N, Corris PA, Frost A, et al. Updated treatment algorithm of pulmonary arterial hypertension. J Am Coll Cardiol 2013; 62(25 Suppl): D60–72. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
