

Mortality after emergent trauma laparotomy: A multicenter, retrospective study
- PMID: 28598906
- PMCID: PMC5573610
- DOI: 10.1097/TA.0000000000001619
Mortality after emergent trauma laparotomy: A multicenter, retrospective study
Abstract
Background: Two decades ago, hypotensive trauma patients requiring emergent laparotomy had a 40% mortality. In the interim, multiple interventions to decrease hemorrhage-related mortality have been implemented but few have any documented evidence of change in outcomes for patients requiring emergent laparotomy. The purpose of this study was to determine current mortality rates for patients undergoing emergent trauma laparotomy.
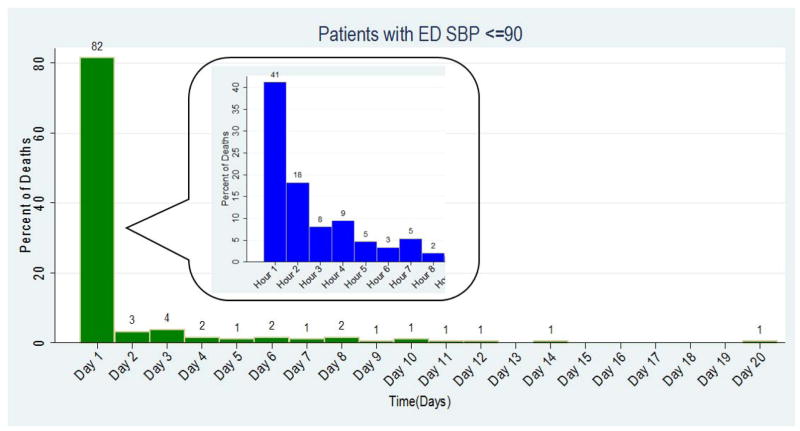
Methods: A retrospective cohort of all adult, emergent trauma laparotomies performed in 2012 to 2013 at 12 Level I trauma centers was reviewed. Emergent trauma laparotomy was defined as emergency department (ED) admission to surgical start time in 90 minutes or less. Hypotension was defined as arrival ED systolic blood pressure (SBP) ≤90 mm Hg. Cause and time to death was also determined. Continuous data are presented as median (interquartile range [IQR]).
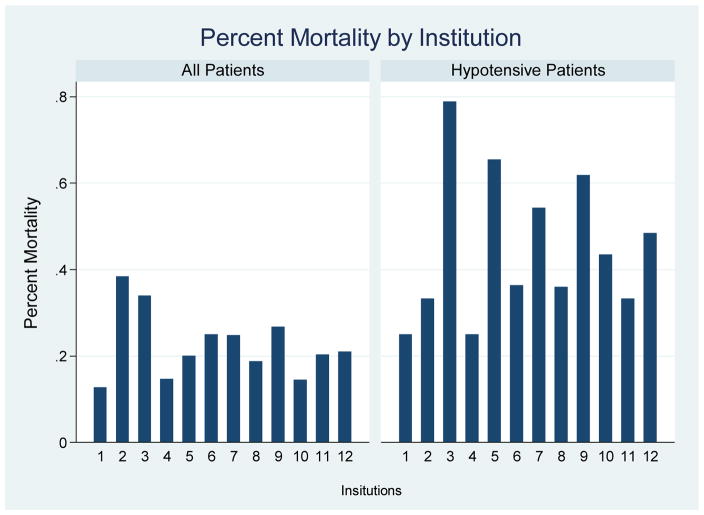
Results: One thousand seven hundred six patients underwent emergent trauma laparotomy. The cohort was predominately young (31 years; IQR, 24-45), male (84%), sustained blunt trauma (67%), and with moderate injuries (Injury Severity Score, 19; IQR, 10-33). The time in ED was 24 minutes (IQR, 14-39) and time from ED admission to surgical start was 42 minutes (IQR, 30-61). The most common procedures were enterectomy (23%), hepatorrhaphy (20%), enterorrhaphy (16%), and splenectomy (16%). Damage control laparotomy was used in 38% of all patients and 62% of hypotensive patients. The Injury Severity Score for the entire cohort was 19 (IQR, 10-33) and 29 (IQR, 18-41) for the hypotensive group. Mortality for the entire cohort was 21% with 60% of deaths due to hemorrhage. Mortality in the hypotensive group was 46%, with 65% of deaths due to hemorrhage.
Conclusion: Overall mortality rate of a trauma laparotomy is substantial (21%) with hemorrhage accounting for 60% of the deaths. The mortality rate for hypotensive patients (46%) appears unchanged over the last two decades and is even more concerning, with almost half of patients presenting with an SBP of 90 mm Hg or less dying.
Figures
References
-
- Cothren CC, Moore EE, Hedegaard HB, Meng K. Epidemiology of Urban Trauma Deaths: a Comprehensive Reassessment 10 Years Later. World J Surg. 2007 Jul;31(7):1507–11. - PubMed
-
- Hoyt DB, Shackford SR, McGill T, Mackersie R, Davis J, Hansbrough J. The Impact of In-House Surgeons and Operating Room Resuscitation on Outcomes of Traumatic Injuries. Arch Surg. 1989 Aug;124(8):906–09. - PubMed
-
- Steele JT, Hoyt DB, Simons RK, Winchell RJ, Garcia J, Fortlage BA. Is Operating Room Resuscitation a Way to Save Time? Am J Surg. 1997 Dec;174(6):683–87. - PubMed
-
- Clarke JR, Trooskin SZ, Doshi PJ, Greenwald L, Mode CL. Time to Laparotomy for Intra-Abdominal Bleeding form Trauma Does Affect Survival for Delays up to 90 Minutes. J Trauma. 2002;52(3):420–425. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
