

Multipolar pacing by cardiac resynchronization therapy with a defibrillators treatment in type 2 diabetes mellitus failing heart patients: impact on responders rate, and clinical outcomes
- PMID: 28599667
- PMCID: PMC5466779
- DOI: 10.1186/s12933-017-0554-2
Multipolar pacing by cardiac resynchronization therapy with a defibrillators treatment in type 2 diabetes mellitus failing heart patients: impact on responders rate, and clinical outcomes
Abstract
Background: Type 2 diabetes mellitus (T2DM) is a multi factorial disease, affecting clinical outcomes in failing heart patients treated by cardiac resynchronization therapy with a defibrillator (CRT-d).
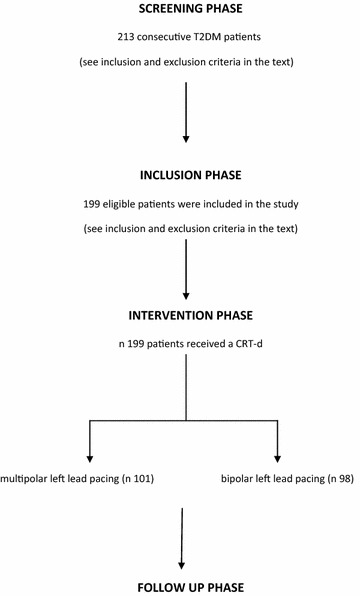
Methods: One hundred and ninety-five T2DM patients received a CRT-d treatment. Randomly the study population received a CRT-d via multipolar left ventricle (LV) lead pacing (n 99, multipolar group), vs a CRT-d via bipolar LV pacing (n 96, bipolar group). These patients were followed by clinical, and instrumental assessment, and telemetric device control at follow up. In this study we evaluated, in a population of failing heart T2DM patients, cardiac deaths, all cause deaths, arrhythmic events, CRT-d responders rate, hospitalizations for HF worsening, phrenic nerve stimulation (PNS), and LV catheter dislodgment events (and re-intervention for LV catheter re-positioning), comparing multipolar CRT-d vs bipolar CRT-d group of patients at follow up.
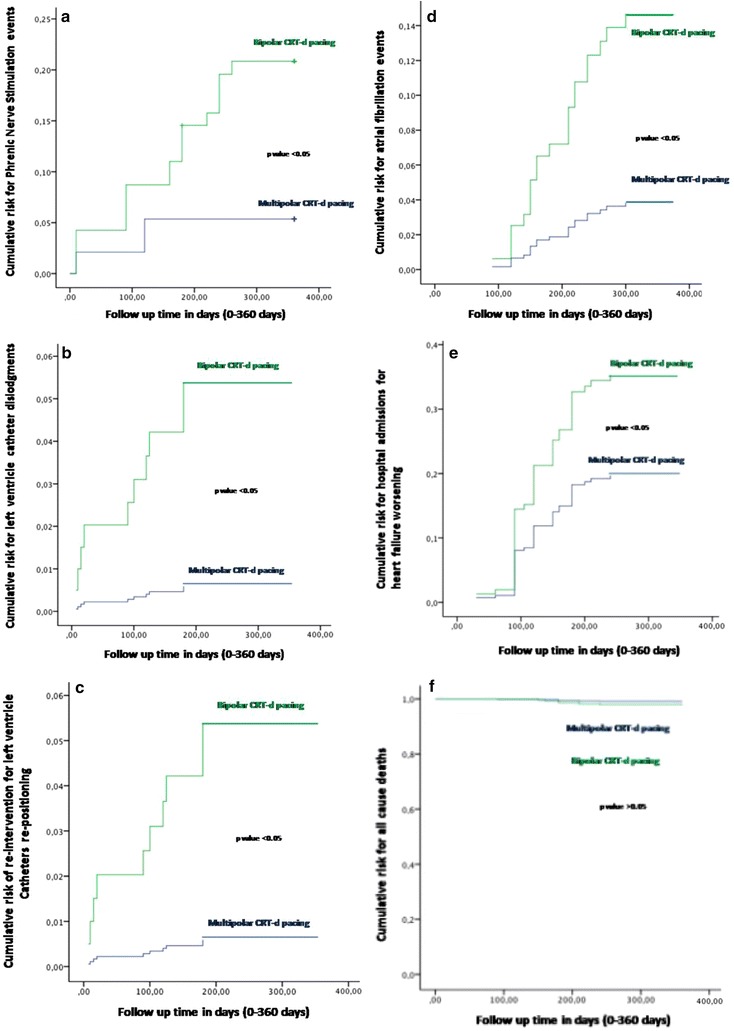
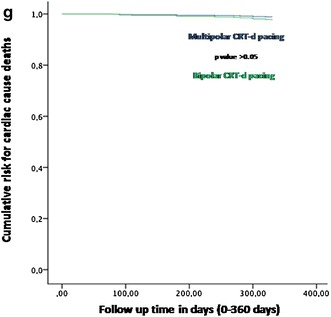
Results: At follow up there was a statistical significant difference about atrial arrhythmic events [7 (7%) vs 16 (16.7%), p value 0.019], hospitalizations for HF worsening [15 (15.2% vs 24 (25%), p value 0.046], LV catheter dislodgments [1 (1%) vs 9 (9.4%), p value 0018], PNS [5 (5%) vs 18 (18.7%), p value 0.007], and LV re-positioning [1 (1%) vs 9 (9.4%), p value 0.018], comparing multipolar CRT-d vs bipolar CRT-d group of patients. Multipolar pacing was an independent predictor of all these events.
Conclusions: CRT-d pacing via multipolar LV lead vs bipolar LV lead may reduce arrhythmic burden, hospitalization rate, PNS, LV catheters dislodgments, and re-interventions in T2DM failing heart patients. Clinical trial number NCT03095196.
Figures
References
-
- Moss AJ, Jackson Hall W, Cannom DS, Klein H, Brown MW, James WS, Daubert P, Mark Estes NA, Foster E, Greenberg H, Higgins SL, Pfeffer MA, Solomon SD, Wilber D, Zareba W, for the MADIT-CRT Trial Investigators* Cardiac-resynchronization therapy for the prevention of heart-failure events. N Engl J Med. 2009;361:1329–1338. doi: 10.1056/NEJMoa0906431. - DOI - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
