

Markers of Successful Extubation in Extremely Preterm Infants, and Morbidity After Failed Extubation
- PMID: 28600154
- PMCID: PMC5657557
- DOI: 10.1016/j.jpeds.2017.04.050
Markers of Successful Extubation in Extremely Preterm Infants, and Morbidity After Failed Extubation
Abstract
Objectives: To identify variables associated with successful elective extubation, and to determine neonatal morbidities associated with extubation failure in extremely preterm neonates.
Study design: This study was a secondary analysis of the National Institute of Child Health and Human Development Neonatal Research Network's Surfactant, Positive Pressure, and Oxygenation Randomized Trial that included extremely preterm infants born at 240/7 to 276/7 weeks' gestation. Patients were randomized either to a permissive ventilatory strategy (continuous positive airway pressure group) or intubation followed by early surfactant (surfactant group). There were prespecified intubation and extubation criteria. Extubation failure was defined as reintubation within 5 days of extubation.
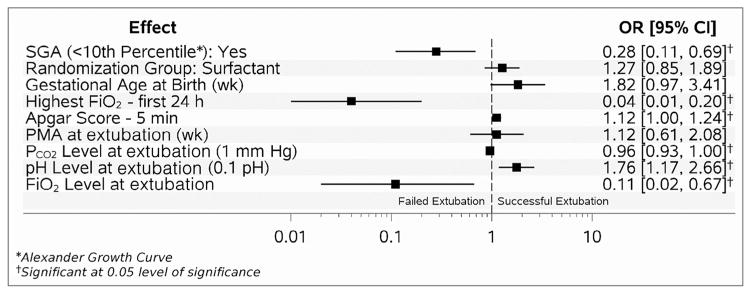
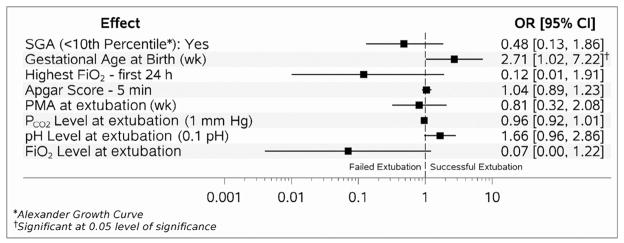
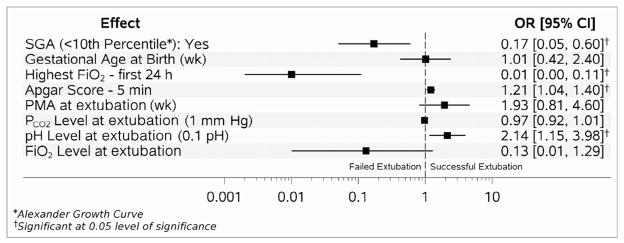
Results: Of 1316 infants in the trial, 1071 were eligible; 926 infants had data available on extubation status; 538 were successful and 388 failed extubation. The rate of successful extubation was 50% (188/374) in the continuous positive airway pressure group and 63% (350/552) in the surfactant group. Successful extubation was associated with higher 5-minute Apgar score, and pH prior to extubation, lower peak fraction of inspired oxygen within the first 24 hours of age and prior to extubation, lower partial pressure of carbon dioxide prior to extubation, and non-small for gestational age status after adjustment for the randomization group assignment. Infants who failed extubation had higher adjusted rates of mortality (OR 2.89), bronchopulmonary dysplasia (OR 3.06), and death/ bronchopulmonary dysplasia (OR 3.27).
Conclusions: Higher 5-minute Apgar score, and pH prior to extubation, lower peak fraction of inspired oxygen within first 24 hours of age, lower partial pressure of carbon dioxide and fraction of inspired oxygen prior to extubation, and nonsmall for gestational age status were associated with successful extubation. Failed extubation was associated with significantly higher likelihood of mortality and morbidities.
Trial registration: ClinicalTrials.gov: NCT00233324.
Keywords: bronchopulmonary dysplasia; extremely preterm; extubation; neonatal morbidity.
Copyright © 2017 Elsevier Inc. All rights reserved.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures

Comment in
-
Solving the Extubation Equation: Successfully Weaning Infants Born Extremely Preterm from Mechanical Ventilation.J Pediatr. 2017 Oct;189:17-18. doi: 10.1016/j.jpeds.2017.06.015. Epub 2017 Jul 10. J Pediatr. 2017. PMID: 28705653 No abstract available.
-
Reply.J Pediatr. 2018 Mar;194:263-264. doi: 10.1016/j.jpeds.2017.11.017. Epub 2017 Dec 6. J Pediatr. 2018. PMID: 29221692 No abstract available.
-
Deciphering extubation failure in extremely preterm infants: Time to embrace complexity and move forward.J Pediatr. 2018 Mar;194:263. doi: 10.1016/j.jpeds.2017.11.016. Epub 2017 Dec 13. J Pediatr. 2018. PMID: 29248182 No abstract available.
References
-
- Walsh MC, Morris BH, Wrage LA, Vohr BR, Poole WK, Tyson JE, et al. Extremely low birthweight neonates with protracted ventilation: mortality and 18-month neurodevelopmental outcomes. J Pediatr. 2005;146:798–804. - PubMed
-
- Bancalari E, Gerhardt T. Bronchopulmonary dysplasia. Pediatr Clin North Am. 1986;33:1–23. - PubMed
-
- Strong RM, Passy V. Endotracheal intubation. Complications in neonates. Arch Otolaryngol. 1977;103:329–35. - PubMed
-
- Morley CJ, Davis PG, Doyle LW, Brion LP, Hascoet JM, Carlin JB. Nasal CPAP or intubation at birth for very preterm infants. N Engl J Med. 2008;358:700–8. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
- U10 HD027856/HD/NICHD NIH HHS/United States
- U10 HD021385/HD/NICHD NIH HHS/United States
- U10 HD053119/HD/NICHD NIH HHS/United States
- U10 HD021364/HD/NICHD NIH HHS/United States
- UG1 HD053089/HD/NICHD NIH HHS/United States
- U10 HD040461/HD/NICHD NIH HHS/United States
- U10 HD040492/HD/NICHD NIH HHS/United States
- UG1 HD027856/HD/NICHD NIH HHS/United States
- UG1 HD034216/HD/NICHD NIH HHS/United States
- U10 HD027871/HD/NICHD NIH HHS/United States
- UG1 HD027904/HD/NICHD NIH HHS/United States
- U10 HD027851/HD/NICHD NIH HHS/United States
- UG1 HD027880/HD/NICHD NIH HHS/United States
- UG1 HD053109/HD/NICHD NIH HHS/United States
- UG1 HD027851/HD/NICHD NIH HHS/United States
- U10 HD040498/HD/NICHD NIH HHS/United States
- U10 HD053089/HD/NICHD NIH HHS/United States
- UG1 HD087226/HD/NICHD NIH HHS/United States
- U10 HD053124/HD/NICHD NIH HHS/United States
- U10 HD027880/HD/NICHD NIH HHS/United States
- UG1 HD027853/HD/NICHD NIH HHS/United States
- U10 HD040521/HD/NICHD NIH HHS/United States
- U10 HD053109/HD/NICHD NIH HHS/United States
- UG1 HD087229/HD/NICHD NIH HHS/United States
- UG1 HD040689/HD/NICHD NIH HHS/United States
- U10 HD027853/HD/NICHD NIH HHS/United States
- U10 HD027904/HD/NICHD NIH HHS/United States
- U10 HD021397/HD/NICHD NIH HHS/United States
- UG1 HD040492/HD/NICHD NIH HHS/United States
- UG1 HD021364/HD/NICHD NIH HHS/United States
- U10 HD034216/HD/NICHD NIH HHS/United States
- U10 HD036790/HD/NICHD NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
