

Accelerated versus standard epirubicin followed by cyclophosphamide, methotrexate, and fluorouracil or capecitabine as adjuvant therapy for breast cancer in the randomised UK TACT2 trial (CRUK/05/19): a multicentre, phase 3, open-label, randomised, controlled trial
- PMID: 28600210
- PMCID: PMC5489700
- DOI: 10.1016/S1470-2045(17)30404-7
Accelerated versus standard epirubicin followed by cyclophosphamide, methotrexate, and fluorouracil or capecitabine as adjuvant therapy for breast cancer in the randomised UK TACT2 trial (CRUK/05/19): a multicentre, phase 3, open-label, randomised, controlled trial
Abstract
Background: Adjuvant chemotherapy for early breast cancer has improved outcomes but causes toxicity. The UK TACT2 trial used a 2×2 factorial design to test two hypotheses: whether use of accelerated epirubicin would improve time to tumour recurrence (TTR); and whether use of oral capecitabine instead of cyclophosphamide would be non-inferior in terms of patients' outcomes and would improve toxicity, quality of life, or both.
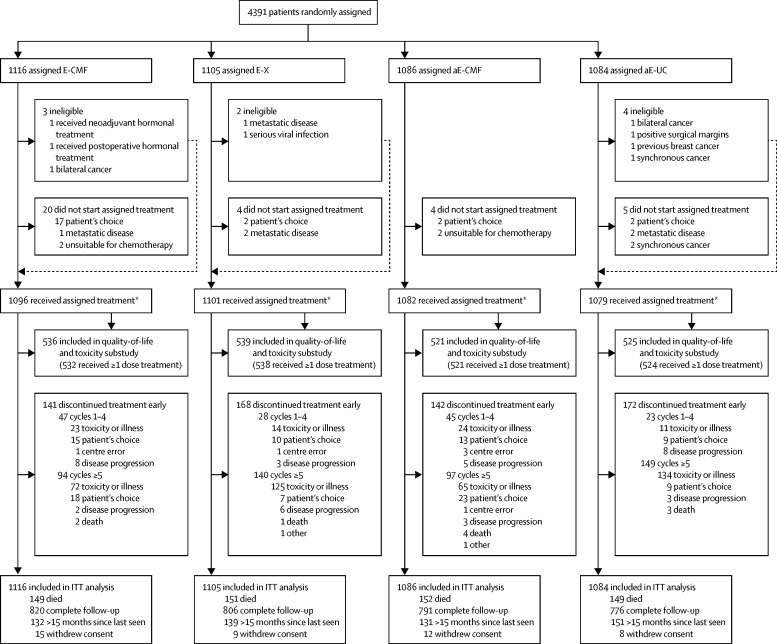
Methods: In this multicentre, phase 3, randomised, controlled trial, we enrolled patients aged 18 years or older from 129 UK centres who had histologically confirmed node-positive or high-risk node-negative operable breast cancer, had undergone complete excision, and were due to receive adjuvant chemotherapy. Patients were randomly assigned to receive four cycles of 100 mg/m2 epirubicin either every 3 weeks (standard epirubicin) or every 2 weeks with 6 mg pegfilgrastim on day 2 of each cycle (accelerated epirubicin), followed by four 4-week cycles of either classic cyclophosphamide, methotrexate, and fluorouracil (CMF; 600 mg/m2 cyclophosphamide intravenously on days 1 and 8 or 100 mg/m2 orally on days 1-14; 40 mg/m2 methotrexate intravenously on days 1 and 8; and 600 mg/m2 fluorouracil intravenously on days 1 and 8 of each cycle) or four 3-week cycles of 2500 mg/m2 capecitabine (1250 mg/m2 given twice daily on days 1-14 of each cycle). The randomisation schedule was computer generated in random permuted blocks, stratified by centre, number of nodes involved (none vs one to three vs four or more), age (≤50 years vs >50 years), and planned endocrine treatment (yes vs no). The primary endpoint was TTR, defined as time from randomisation to first invasive relapse or breast cancer death, with intention-to-treat analysis of standard versus accelerated epirubicin and per-protocol analysis of CMF versus capecitabine. This trial is registered with ISRCTN, number 68068041, and with ClinicalTrials.gov, number NCT00301925.
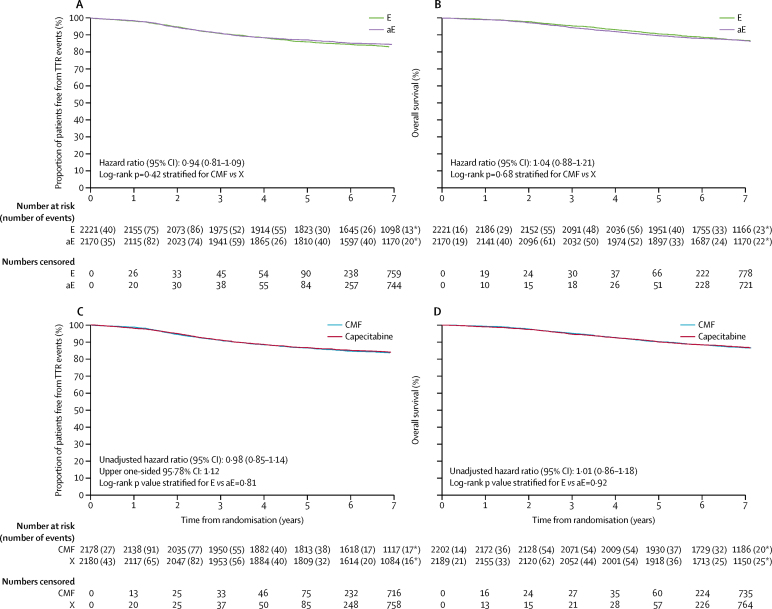
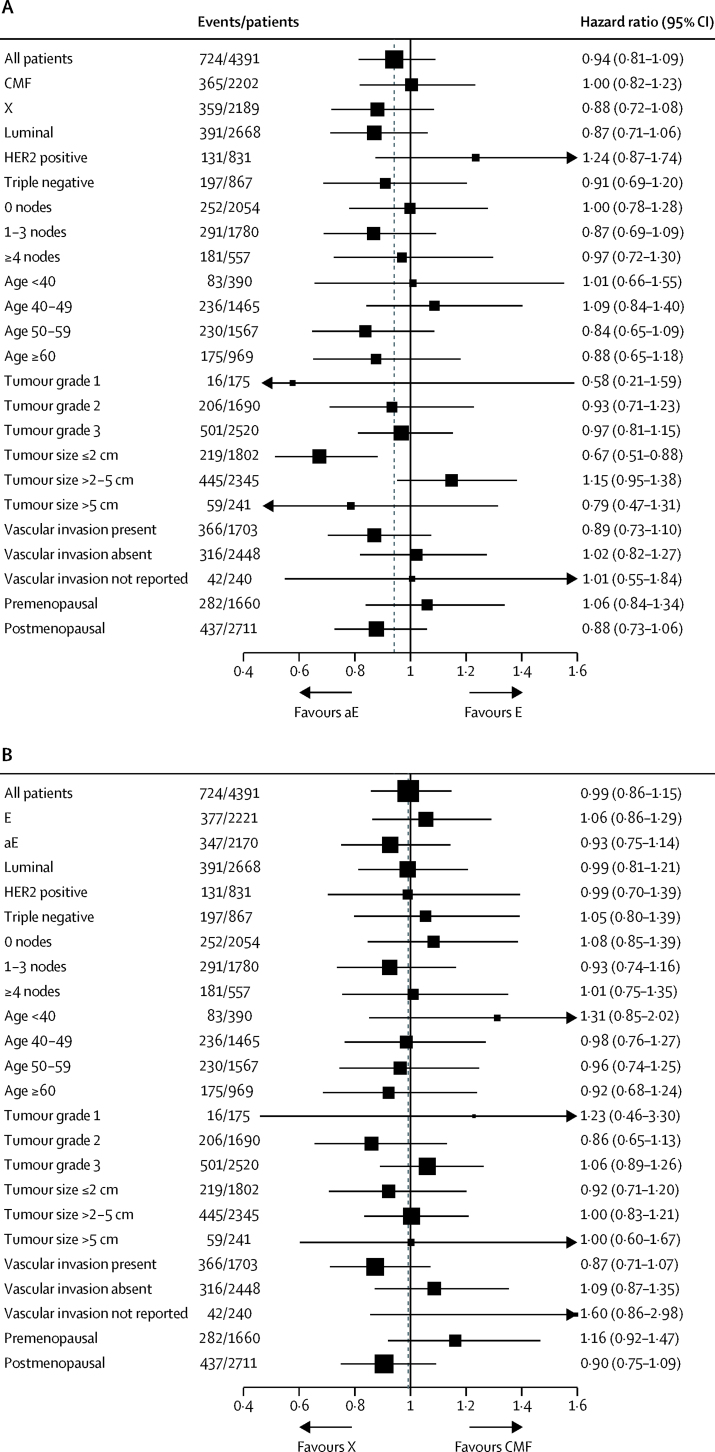
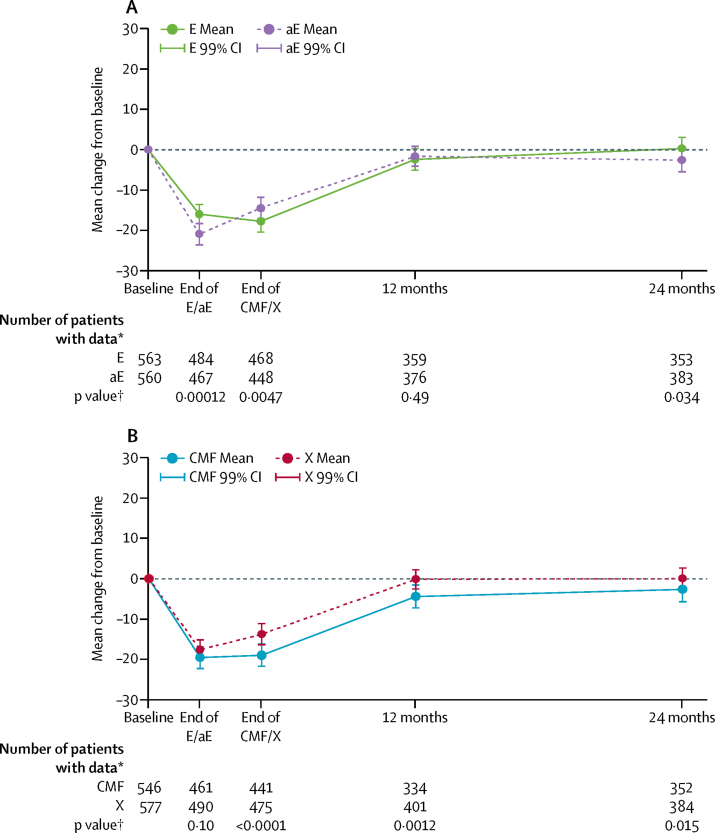
Findings: From Dec 16, 2005, to Dec 5, 2008, 4391 patients (4371 women and 20 men) were recruited. At a median follow-up of 85·6 months (IQR 80·6-95·9) no significant difference was seen in the proportions of patients free from TTR events between the accelerated and standard epirubicin groups (overall hazard ratio [HR] 0·94, 95% CI 0·81-1·09; stratified p=0·42). At 5 years, 85·9% (95% CI 84·3-87·3) of patients receiving standard epirubicin and 87·1% (85·6-88·4) of those receiving accelerated epirubicin were free from TTR events. 4358 patients were included in the per-protocol analysis, and no difference was seen in the proportions of patients free from TTR events between the CMF and capecitabine groups (HR 0·98, 95% CI 0·85-1.14; stratified p=0·00092 for non-inferiority). Compared with baseline, significantly more patients taking CMF than those taking capecitabine had clinically relevant worsening of quality of life at end of treatment (255 [58%] of 441 vs 235 [50%] of 475; p=0·011) and at 12 months (114 [34%] of 334 vs 89 [22%] of 401; p<0·001 at 12 months) and had worse quality of life over time (p<0·0001). Detailed toxicity and quality-of-life data were collected from 2115 (48%) of treated patients. The most common grade 3 or higher adverse events in cycles 1-4 were neutropenia (175 [16%]) and fatigue (56 [5%]) of the 1070 patients treated with standard epirubicin, and fatigue (63 [6%]) and infection (34 [3%]) of the 1045 patients treated with accelerated epirubicin. In cycles 5-8, the most common grade 3 or higher adverse events were neutropenia (321 [31%]) and fatigue (109 [11%]) in the patients treated with CMF, and hand-foot syndrome (129 [12%]) and diarrhoea (67 [6%]) in the 1044 patients treated with capcitabine.
Interpretation: We found no benefit from increasing the dose density of the anthracycline component of chemotherapy. However, capecitabine could be used in place of CMF without significant loss of efficacy and with improved quality of life.
Funding: Cancer Research UK, Amgen, Pfizer, and Roche.
Copyright © 2017 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY license. Published by Elsevier Ltd.. All rights reserved.
Figures
Comment in
-
TACT2: improving treatment tolerability in early breast cancer.Lancet Oncol. 2017 Jul;18(7):843-845. doi: 10.1016/S1470-2045(17)30437-0. Lancet Oncol. 2017. PMID: 28677561 No abstract available.
References
-
- Early Breast Cancer Trialists' Collaborative Group Effects of chemotherapy and hormonal therapy for early breast cancer on recurrence and 15-year survival: an overview of the randomised trials. Lancet. 2005;365:1687–1717. - PubMed
-
- Citron ML, Berry DA, Cirrincione C. Randomized trial of dose-dense versus conventionally scheduled and sequential versus concurrent combination chemotherapy as postoperative adjuvant treatment of node-positive primary breast cancer: first report of Intergroup Trial C9741/Cancer and Leukemia Group B Trial 9741. J Clin Oncol. 2003;21:1431–1439. - PubMed
-
- Martin M, Rodriguez-Lescure A, Ruiz A. Randomized phase 3 trial of fluorouracil, epirubicin, and cyclophosphamide alone or followed by paclitaxel for early breast cancer. J Natl Cancer Inst. 2008;100:805–814. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
