

Specialist Endoscopists Are Associated with a Decreased Risk of Incomplete Polyp Resection During Endoscopic Mucosal Resection in the Colon
- PMID: 28600656
- PMCID: PMC6049819
- DOI: 10.1007/s10620-017-4643-6
Specialist Endoscopists Are Associated with a Decreased Risk of Incomplete Polyp Resection During Endoscopic Mucosal Resection in the Colon
Abstract
Background: Endoscopic experience is known to correlate with outcomes of endoscopic mucosal resection (EMR), particularly complete resection of the polyp tissue. Whether specialist endoscopists can protect against incomplete polypectomy in the setting of known risk factors for incomplete resection (IR) is unknown.
Aims: We aimed to characterize how specialist endoscopists may help to mitigate the risk of IR of large sessile polyps.
Methods: This is a retrospective cohort study of patients who underwent EMR at the University of Michigan from January 1, 2006, to November 15, 2015. The primary outcome was endoscopist-reported polyp tissue remaining at the end of the initial EMR attempt. Specialist endoscopists were defined as endoscopists who receive tertiary referrals for difficult colonoscopy cases and completed at least 20 EMR colonic polyp resections over the study period.
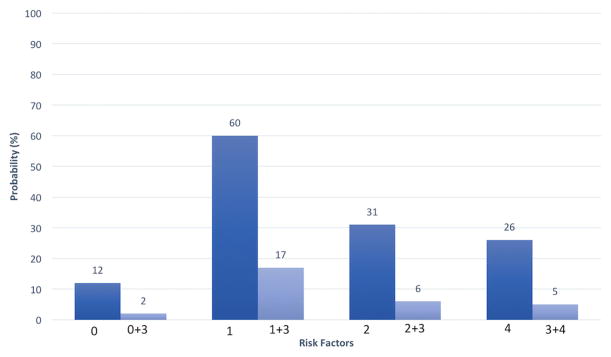
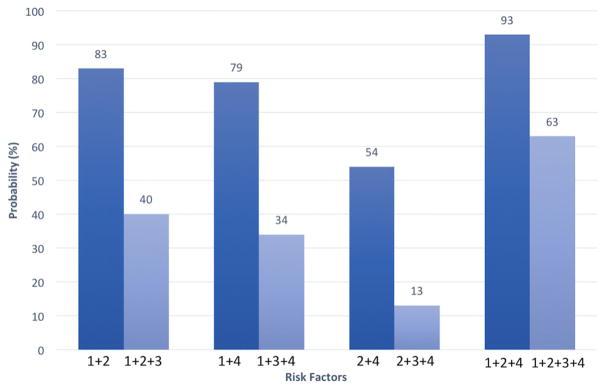
Results: A total of 257 patients with 269 polyps were included in the study. IR occurred in 40 (16%) cases. IR was associated with polyp size ≥ 40 mm [adjusted odds ratio (aOR) 3.31, 95% confidence interval (CI) 1.38-7.93], flat/laterally spreading polyps (aOR 2.61, 95% CI 1.24-5.48), and difficulty lifting the polyp (aOR 11.0, 95% CI 2.66-45.3). A specialist endoscopist performing the initial EMR was protective against IR, even in the setting of risk factors for IR (aOR 0.13, 95% CI 0.04-0.41).
Conclusions: IR is associated with polyp size ≥ 40 mm, flat and/or laterally spreading polyps, and difficulty lifting the polyp. A specialist endoscopist initiating the EMR was protective of IR.
Keywords: Colon; Endoscopic mucosal resection; Polypectomy.
Figures
References
-
- Holt BA, Bourke MJ. Wide field endoscopic resection for advanced colonic mucosal neoplasia: current status and future directions. Clin Gastroenterol Hepatol. 2012;10:969–979. - PubMed
-
- ASGE Technology Committee. Hwang JH, Konda V, et al. Endoscopic mucosal resection. Gastrointest Endosc. 2015;82:215–226. - PubMed
-
- Klein A, Bourke MJ. Advanced polypectomy and resection techniques. Gastrointest Endosc Clin N Am. 2015;25:303–333. - PubMed
-
- Saunders BP, Tsiamoulos ZP. Endoscopic mucosal resection and endoscopic submucosal dissection of large colonic polyps. Nat Rev Gastroenterol Hepatol. 2016;13:486–496. - PubMed
-
- Keswani RN, Law R, Ciolino JD, et al. Adverse events after surgery for nonmalignant colon polyps are common and associated with increased length of stay and costs. Gastrointest Endosc. 2016;84:296e1–303.e1. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
