

Restricted Ventilation Associated with Reduced Neurodevelopmental Impairment in Preterm Infants
- PMID: 28601870
- PMCID: PMC5637296
- DOI: 10.1159/000471841
Restricted Ventilation Associated with Reduced Neurodevelopmental Impairment in Preterm Infants
Abstract
Background and objective: Restrictive use of invasive mechanical ventilation (IMV) in preterm infants reduces the risk of bronchopulmonary dysplasia (BPD). Our objective was to determine its effect on neurodevelopmental impairment (NDI) at 24 months' corrected age (CA).
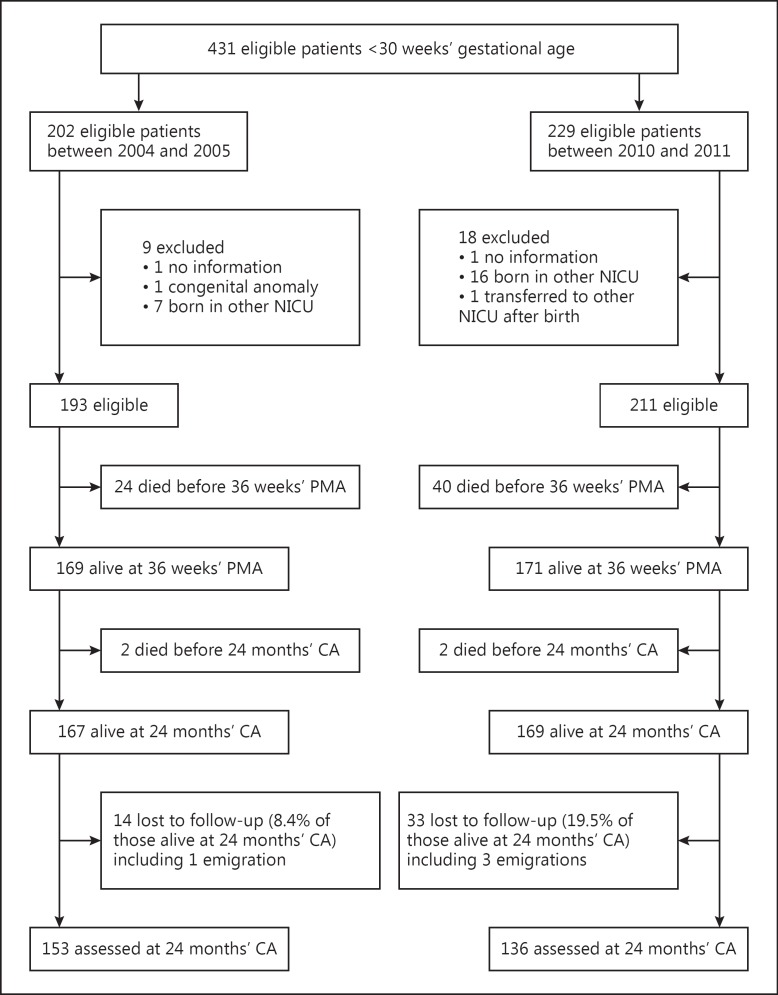
Methods: This retrospective single-center cohort study included all patients with a gestational age <30 weeks born in 2004/2005 (epoch 1) and 2010/2011 (epoch 2). In epoch 2, we introduced a policy of restriction on IMV and liberalized the use of respiratory stimulants in the delivery room and neonatal intensive care. Data on patient characteristics, respiratory management, short-term outcomes, mortality, BPD, and NDI at 24 months' CA were collected.
Results: Four hundred and four preterm infants were included. Compared to those in epoch 1, infants in epoch 2 were less likely to be intubated and the duration of IMV was shorter. Other noninvasive adjuvant therapies such as caffeine, doxapram, and nasal ventilation were more often used during epoch 2. There was a trend to less BPD in epoch 2 compared to epoch 1 (17 vs. 23%, adjusted OR = 0.75, 95% CI: 0.48, 1.16). Mortality did not change over time. The combined outcome death or NDI at 24 months' CA was significantly lower in epoch 2 compared to epoch 1 (24.7 vs. 33.9%, adjusted OR = 0.71, 95% CI: 0.53, 0.97).
Conclusions: Restricted use of IMV is feasible in preterm infants and might be associated with a reduced risk of the combined outcome death or NDI at 24 months' CA. Larger studies are needed to confirm these findings.
Keywords: Bronchopulmonary dysplasia; Invasive mechanical ventilation; Neurodevelopmental impairment.
© 2017 The Author(s) Published by S. Karger AG, Basel.
Figures
References
-
- Soll RF, Edwards EM, Badger GJ, Kenny MJ, Morrow KA, Buzas JS, et al. Obstetric and neonatal care practices for infants 501-1,500 g from 2000 to 2009. Pediatrics. 2013;132:222–228. - PubMed
-
- Miller JD, Carlo WA. Pulmonary complications of mechanical ventilation in neonates. Clin Perinatol. 2008;35:273–281. - PubMed
-
- Jobe AH, Bancalari E. Bronchopulmonary dysplasia. Am J Respir Crit Care Med. 2001;163:1723–1729. - PubMed
-
- Ehrenkranz RA, Walsh MC, Vohr BR, Jobe AH, Wright LL, Fanaroff AA, et al. Validation of the National Institutes of Health consensus definition of bronchopulmonary dysplasia. Pediatrics. 2005;116:1353–1360. - PubMed
-
- Walsh MC, Morris BH, Wrage LA, Vohr BR, Poole WK, Tyson JE, et al. Extremely low birthweight neonates with protracted ventilation: mortality and 18-month neurodevelopmental outcomes. J Pediatr. 2005;146:798–804. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
