

Empathic Care and Distress: Predictive Brain Markers and Dissociable Brain Systems
- PMID: 28602689
- PMCID: PMC5532453
- DOI: 10.1016/j.neuron.2017.05.014
Empathic Care and Distress: Predictive Brain Markers and Dissociable Brain Systems
Abstract
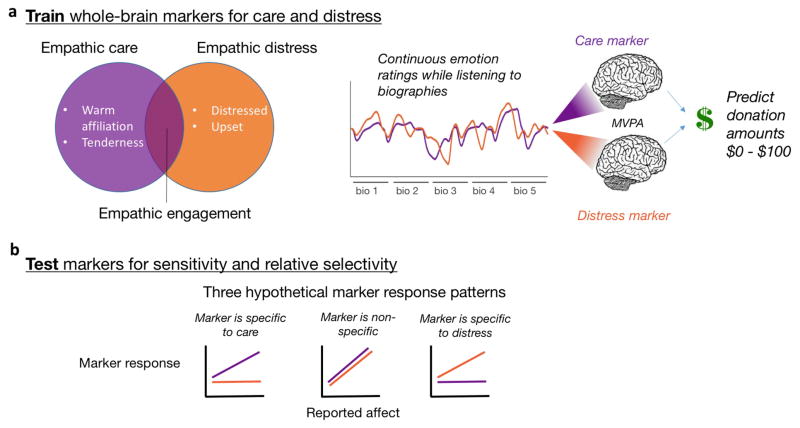
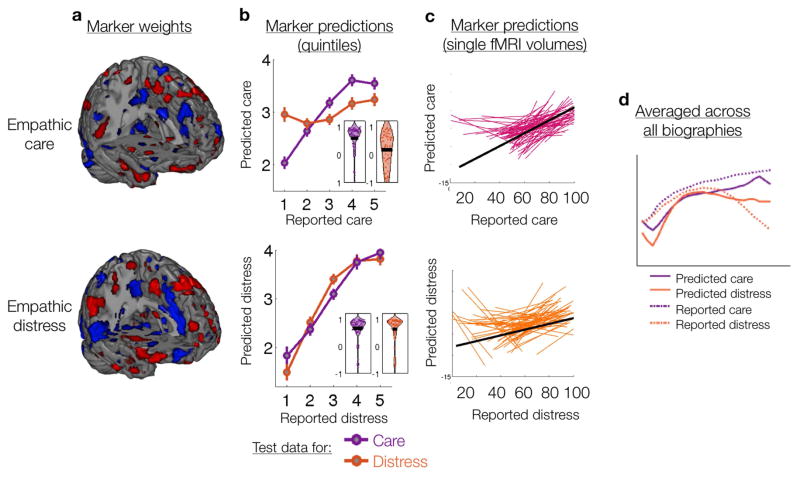
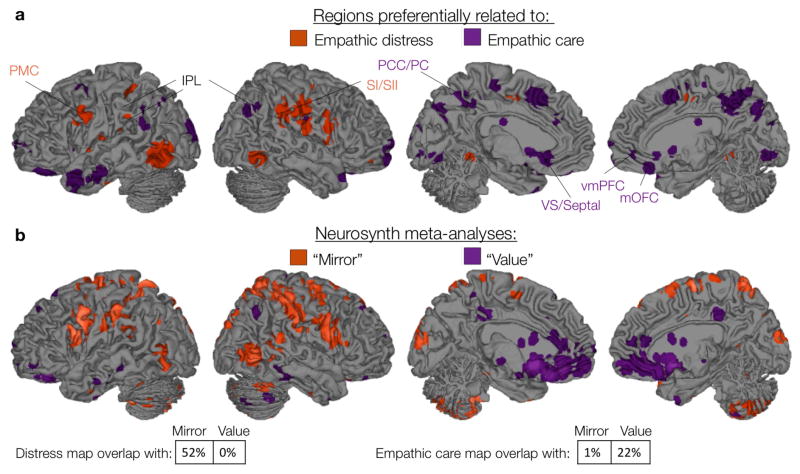
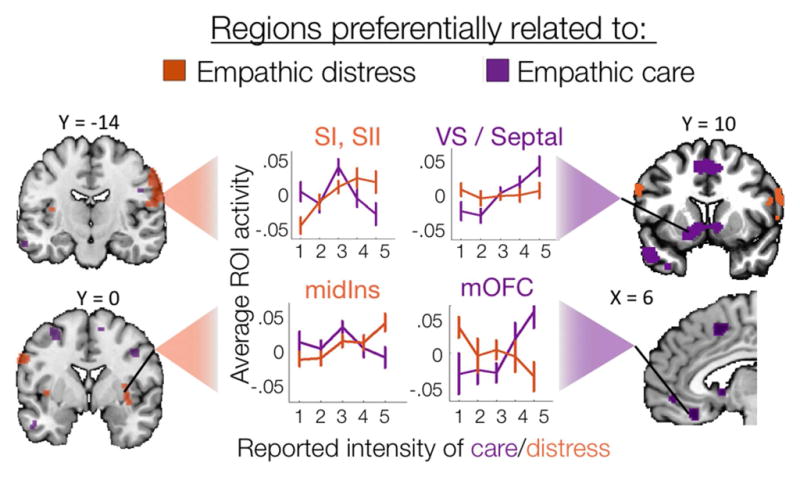
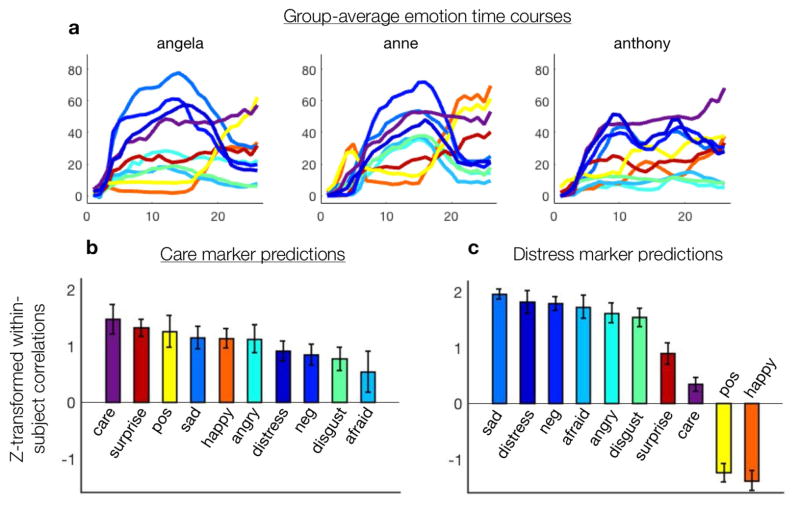
Encountering another's suffering can elicit both empathic distress and empathic care-the warm desire to affiliate. It remains unclear whether these two feelings can be accurately and differentially predicted from neural activity and to what extent their neural substrates can be distinguished. We developed fMRI markers predicting moment-by-moment intensity levels of care and distress intensity while participants (n = 66) listened to true biographies describing human suffering. Both markers' predictions correlated strongly with self-report in out-of-sample participants (r = 0.59 and r = 0.63, p < 0.00001), and both markers predicted later trial-by-trial charitable donation amounts (p < 0.05). Empathic care was preferentially associated with nucleus accumbens and medial orbitofrontal cortex activity, whereas distress was preferentially associated with premotor and somatosensory cortical activity. In tests of marker specificity with an independent behavioral sample (n = 200), the empathic care marker was associated with a mixed-valence feeling state, whereas the empathic distress marker was specific to negative emotion.
Keywords: altruism; biomarker; compassion; empathy; prosocial.
Copyright © 2017 Elsevier Inc. All rights reserved.
Figures
References
-
- Admon R, Pizzagalli DA. Corticostriatal pathways contribute to the natural time course of positive mood. Nature Communications. 2015;6(May):10065. http://doi.org/10.1038/ncomms10065. - DOI - PMC - PubMed
-
- Ashar YK, Andrews-Hanna JR, Dimidjian S, Wager TD. Towards a neuroscience of compassion: A brain systems-based model and research agenda. In: Greene JD, editor. Positive Neuroscience. Oxford University Press; 2016. pp. 1–27.
-
- Ashar YK, Andrews-Hanna JR, Yarkoni T, Sills J, Halifax J, Dimidjian S, Wager TD. Effects of Compassion Meditation on a psychological model of charitable donation. Emotion 2016 - PubMed
-
- Ashar YK, Chang LJ, Wager TD. Mechanisms of the placebo: an affective appraisal account. Annual Reviews Clinical Psychology 2017 - PubMed
-
- Batson CD. Altruism in humans. Oxford University Press; 2011.
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
