

Predicting the Need for Fluid Therapy-Does Fluid Responsiveness Work?
- PMID: 28603624
- PMCID: PMC5461727
- DOI: 10.1186/s40560-017-0210-7
Predicting the Need for Fluid Therapy-Does Fluid Responsiveness Work?
Abstract
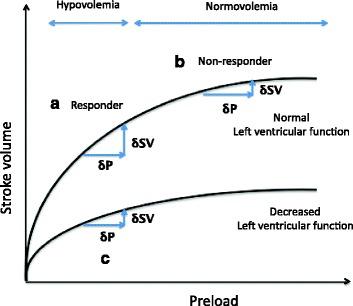
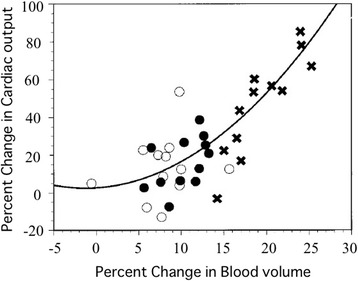
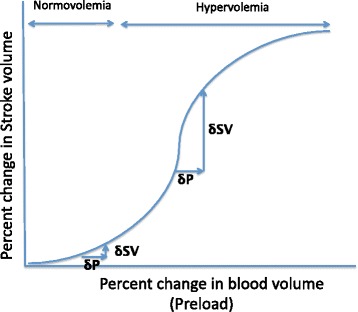
Fluid overdose can be harmful in critically ill patients. Since central venous pressure (CVP) is currently considered to be an inappropriate indicator of preload, much attention is being given to predicting fluid responsiveness, i.e., the response of stroke volume (SV) or cardiac output (CO) to fluid challenge. However, when fluid responsiveness was evaluated in critically ill patients, including sepsis, only 40-50% of the patients responded. Moreover, most fluid responders do not show significant hemodynamic improvement after fluid administration. In this review, we discuss why fluid responsiveness based on the Starling mechanism did not work well in the clinical setting. According to the Starling mechanism, a patient whose SV/CO significantly increases after a fluid challenge is considered to be a fluid responder and judged to need fluid therapy. However, the currently recommended fluid challenge dose of crystalloid 250-500 mL has little effect on increasing blood volume and is not sufficient to increase the preload of the Starling curve. Especially in septic patients, due to their vascular hyperpermeability, increase in blood volume is even smaller. Furthermore, Infusion induced hemodilution is known to reduce blood viscosity and hematocrit, as a result, decreasing afterload. This indicates that the increased SV/CO after fluid challenge is caused not only by increased preload but also by decreased afterload. For these reasons, fluid responsiveness with small crystalloid challenge is questionable as a clinical indicator of fluid therapy.
Keywords: Afterload; Cardiac output; Colloid; Crystalloid; Fluid challenge; Fluid responsiveness; Fluid therapy; Preload; Starling mechanism; Starling’s law; Stroke volume; Systemic vascular resistance.
Figures

References
-
- Rothe CF. Reflex control of veins and vascular capacitance. Physiol Rev. 1983;63(4):1281–342. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
