

Understanding local performance data for EBUS-TBNA: insights from an unselected case series at a high volume UK center
- PMID: 28603645
- PMCID: PMC5459869
- DOI: 10.21037/jtd.2017.05.18
Understanding local performance data for EBUS-TBNA: insights from an unselected case series at a high volume UK center
Abstract
Background: We reviewed the diagnostic performance of endobronchial ultrasound transbronchial aspiration (EBUS-TBNA) on an unselected large cohort of patients who underwent the procedure in our institution in the past 3 years and to compare against published standards and existing literature.
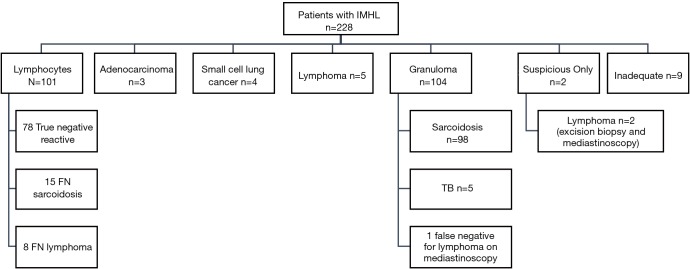
Methods: All consecutive patients who underwent EBUS from January 2013 to December 2015 were included in the retrospective analysis, with a minimum of 6 months of clinico-radiological follow up. For assessing EBUS-TBNA performance, patients were analysed in three subgroups based on the indication for the EBUS-TBNA: in investigation of isolated mediastinal and/or hilar lymphadenopathy (IMHL), in staging of suspected or confirmed non-small cell lung cancer (NSCLC) and in making a tissue diagnosis in suspected thoracic or extrathoracic cancer. For patients subjected to EBUS-TBNA for staging in suspected lung cancer, accuracy of EBUS was measured by its ability to determine the true N2 stage.
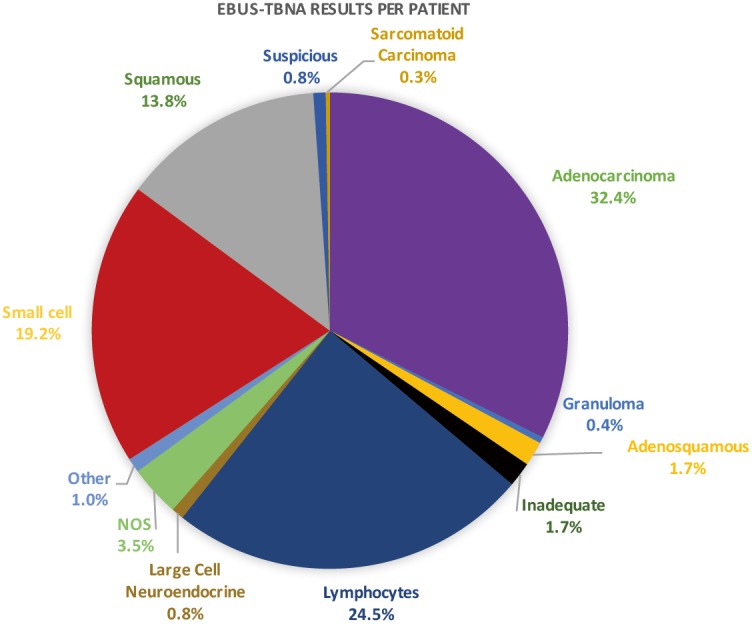
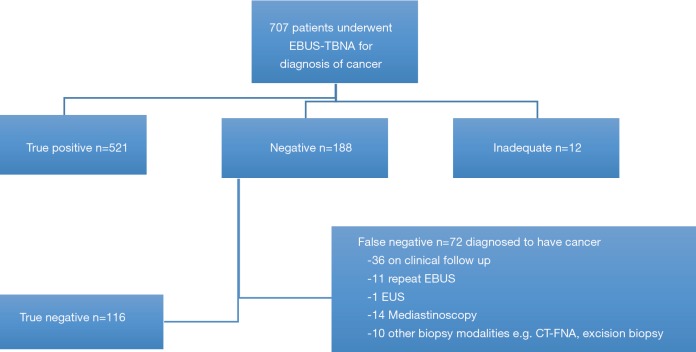
Results: A total of 1,656 lymph nodes and 138 peribronchial/peritracheal masses were sampled in 940 patients over the study period. The prevalence of reactive lymphadenopathy was 34%. The overall sensitivity to detect pathological disease was 81.6% (95% CI: 74.2-87.6%) whilst NPV was 74.8% (95% CI: 65.2-82.8%). Amongst patients who underwent EBUS-TBNA for staging purposes, the sensitivity for N2 staging was 83.7% (95% CI: 76.2-89.6%) and NPV was 81.6% (95% CI: 73.2-88.2%). The prevalence of N2 disease was 58%. In the subgroup of patients who proceeded to surgical sampling, the sensitivity was higher with the N2/N3 disease prevalence of 67.4%. The sensitivity of EBUS-TBNA to make a tissue diagnosis of thoracic or extrathoracic cancer was 88% (95% CI: 85.1-90.5%) and a NPV of 62% (95% CI: 54.7-69.0%). The disease prevalence was 83.6%.
Conclusions: This retrospective study of a large volume of patients represents real life practice and provides an accurate representation of the typical cohort of patients referred in for EBUS-TBNA to the general respiratory physician in UK. Our study highlights the pitfalls in collecting and analyzing data but also demonstrates how they can be used to improve service performance.
Keywords: Endobronchial ultrasound (EBUS); extrathoracic malignancy; lung cancer; mediastinal lymphadenopathy.
Conflict of interest statement
Conflicts of Interest: The authors have no conflicts of interest to declare.
Figures
References
-
- NICE lung cancer guidelines. Available online: https://www.nice.org.uk/guidance/cg121/chapter/1-Guidance.
-
- Silvestri GA, Gonzalez AV, Jantz MA, et al. Methods for staging non-small cell lung cancer diagnosis and management of lung cancer, 3rd ed: American college of chest physicians Evidence-Based clinical practice guidelines. Chest 2013;143:E211-50. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous