

Consensus guidelines for lumbar puncture in patients with neurological diseases
- PMID: 28603768
- PMCID: PMC5454085
- DOI: 10.1016/j.dadm.2017.04.007
Consensus guidelines for lumbar puncture in patients with neurological diseases
Abstract
Introduction: Cerebrospinal fluid collection by lumbar puncture (LP) is performed in the diagnostic workup of several neurological brain diseases. Reluctance to perform the procedure is among others due to a lack of standards and guidelines to minimize the risk of complications, such as post-LP headache or back pain.
Methods: We provide consensus guidelines for the LP procedure to minimize the risk of complications. The recommendations are based on (1) data from a large multicenter LP feasibility study (evidence level II-2), (2) systematic literature review on LP needle characteristics and post-LP complications (evidence level II-2), (3) discussion of best practice within the Joint Programme Neurodegenerative Disease Research Biomarkers for Alzheimer's disease and Parkinson's Disease and Biomarkers for Multiple Sclerosis consortia (evidence level III).
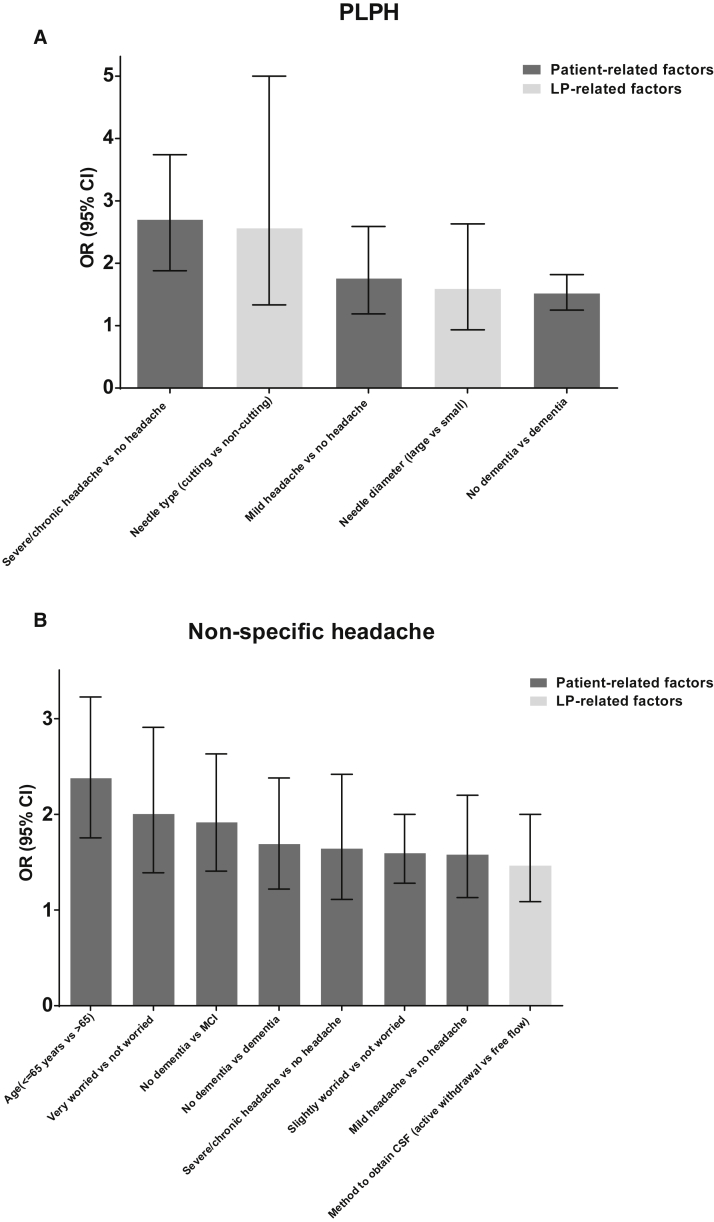
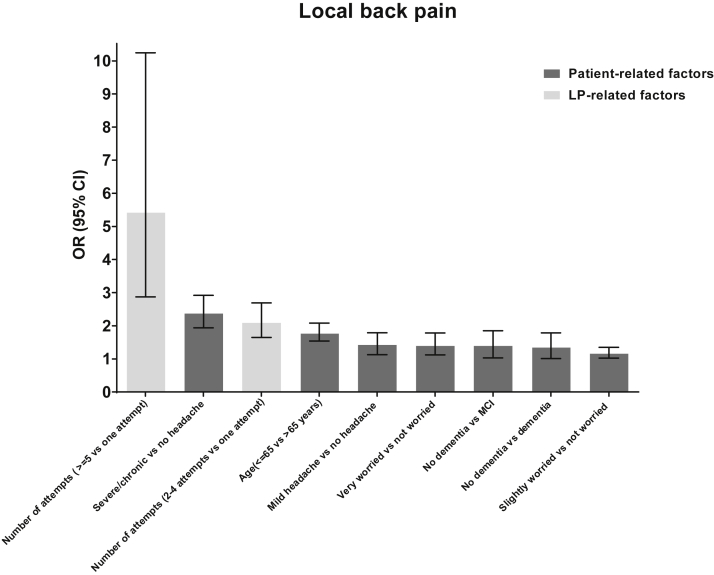
Results: Our consensus guidelines address contraindications, as well as patient-related and procedure-related risk factors that can influence the development of post-LP complications.
Discussion: When an LP is performed correctly, the procedure is well tolerated and accepted with a low complication rate.
Keywords: Back pain; Cerebrospinal fluid; Consensus guidelines; Evidence-based guidelines; Headache; Lumbar puncture; Post-LP complications.
Figures
References
-
- Niemantsverdriet E., Struyfs H., Duits F., Teunissen C., Engelborghs S. Techniques, contraindications and complications of CSF collection procedures. In: Deisenhammer F., Sellebjerg F., Teunissen C.E., Tumani H., editors. Cerebrospinal Fluid in Clinical Neurology. Springer; New York: 2015. pp. 37–57.
-
- McKhann G.M., Knopman D.S., Chertkow H., Hyman B.T., Jack C.R., Jr., Kawas C.H. The diagnosis of dementia due to Alzheimer's disease: recommendations from the National Institute on Aging-Alzheimer's Association workgroups on diagnostic guidelines for Alzheimer's disease. Alzheimers Dement. 2011;7:263–269. - PMC - PubMed
-
- Albert M.S., DeKosky S.T., Dickson D., Dubois B., Feldman H.H., Fox N.C. The diagnosis of mild cognitive impairment due to Alzheimer's disease: recommendations from the National Institute on Aging-Alzheimer's Association workgroups on diagnostic guidelines for Alzheimer's disease. Alzheimers Dement. 2011;7:270–279. - PMC - PubMed
-
- Dubois B., Feldman H.H., Jacova C., Hampel H., Molinuevo J.L., Blennow K. Advancing research diagnostic criteria for Alzheimer's disease: the IWG-2 criteria. Lancet Neurol. 2014;13:614–629. - PubMed
-
- Duits F.H., Martinez-Lage P., Paquet C., Engelborghs S., Lleo A., Hausner L. Performance and complications of lumbar puncture in memory clinics: Results of the multicenter lumbar puncture feasibility study. Alzheimers Dement. 2016;12:154–163. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases