

Should We Be Testing for Baseline Integrase Resistance in Patients Newly Diagnosed With Human Immunodeficiency Virus?
- PMID: 28605418
- PMCID: PMC5850548
- DOI: 10.1093/cid/cix542
Should We Be Testing for Baseline Integrase Resistance in Patients Newly Diagnosed With Human Immunodeficiency Virus?
Abstract
Background: Current guidelines recommend genotype resistance testing at diagnosis to guide initial selection of antiretroviral therapy (ART). Many standard resistance genotypes exclude testing for resistance to integrase inhibitors ("IR testing"), although this class of drugs is a component of most recommended first-line regimens.
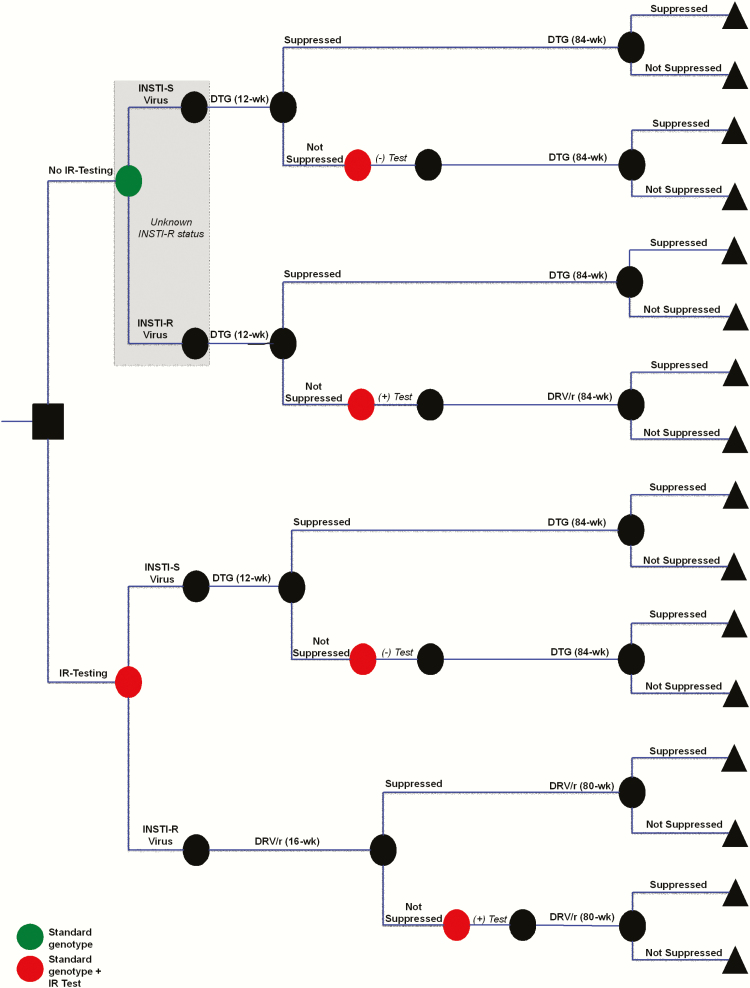
Methods: We compared the 96-week clinical outcomes and cost-effectiveness of 2 strategies: no IR testing vs IR testing performed at human immunodeficiency virus (HIV) diagnosis. The base case prevalence of transmitted integrase strand transfer inhibitor (INSTI)-resistant (INSTI-R) virus is estimated at 0.1%. With no IR testing, all patients start dolutegravir (DTG)-based ART after genotype; 12-week suppression rates are 90% (INSTI-susceptible [INSTI-S] virus) and 35% (INSTI-R virus). Those not suppressed at 12 weeks undergo IR testing; if diagnosed with INSTI-R virus, they change to ritonavir-boosted darunavir (DRV/r)-based ART. With IR testing, all patients are diagnosed with INSTI-S/INSTI-R virus prior to ART initiation and start DTG- or DRV/r-based regimens, respectively. Costs include IR tests (175 US dollars [USD]) and ART (41100-44900 USD/year). We examined the impact of key parameters in sensitivity analyses.
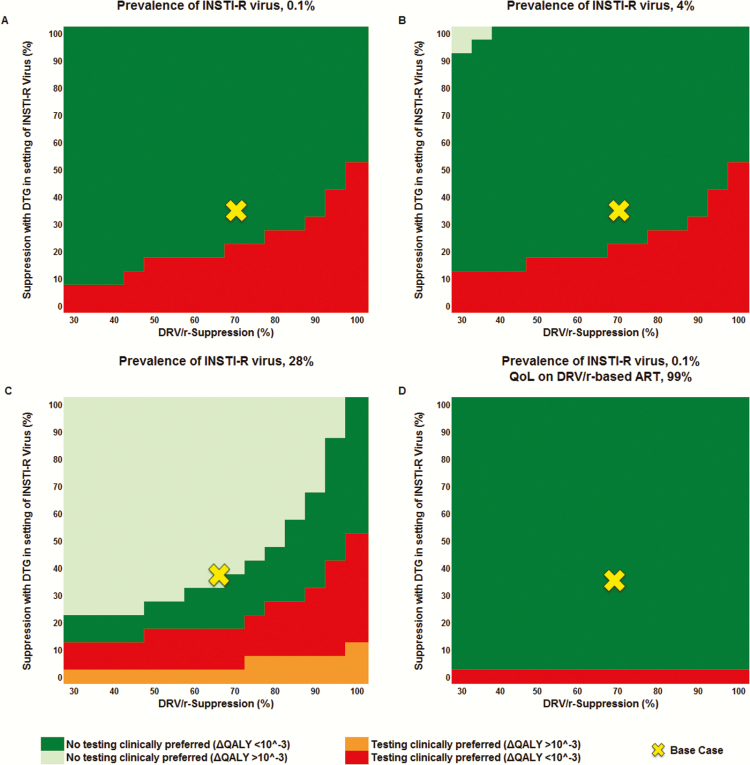
Results: IR testing resulted in worse clinical outcomes compared to no IR testing and increased costs by 200 USD/person/year. Prevalence of transmitted INSTI-R virus did not affect the favored strategy. No IR testing remained clinically preferred unless DTG suppression of INSTI-R virus was <20% or 96-week DRV/r suppression was >92%. If quality of life was worse with DRV/r- than DTG-based ART, no IR testing was clinically preferred over an even broader range of parameters.
Conclusions: In patients with newly diagnosed HIV, IR testing is projected to result in worse outcomes and is not cost-effective. Pretreatment assessment for INSTI resistance should not be recommended in treatment guidelines.
Keywords: ART-naive; HIV; cost-effectiveness analysis; integrase resistance.
© The Author 2017. Published by Oxford University Press for the Infectious Diseases Society of America. All rights reserved. For permissions, e-mail: journals.permissions@oup.com.
Figures
Comment in
-
The Argument Against Testing for INSTI Resistance in Treatment Naive Patients.Clin Infect Dis. 2018 May 17;66(11):1820-1821. doi: 10.1093/cid/ciy015. Clin Infect Dis. 2018. PMID: 29324987 No abstract available.
Similar articles
-
Clinical Impact and Cost-effectiveness of Genotype Testing at Human Immunodeficiency Virus Diagnosis in the United States.Clin Infect Dis. 2020 Mar 17;70(7):1353-1363. doi: 10.1093/cid/ciz372. Clin Infect Dis. 2020. PMID: 31055599 Free PMC article.
-
Integrase Strand Transfer Inhibitor Resistance Mutations in Antiretroviral Therapy-Naive and Treatment-Experienced HIV Patients in South Korea.AIDS Res Hum Retroviruses. 2019 Feb;35(2):213-216. doi: 10.1089/AID.2018.0213. Epub 2018 Oct 23. AIDS Res Hum Retroviruses. 2019. PMID: 30229661
-
Virological outcomes of various first-line ART regimens in patients harbouring HIV-1 E157Q integrase polymorphism: a multicentre retrospective study.J Antimicrob Chemother. 2023 Dec 1;78(12):2859-2868. doi: 10.1093/jac/dkad319. J Antimicrob Chemother. 2023. PMID: 37856677
-
Switching regimens in virologically suppressed HIV-1-infected patients: evidence base and rationale for integrase strand transfer inhibitor (INSTI)-containing regimens.HIV Med. 2016 Oct;17 Suppl 5:3-16. doi: 10.1111/hiv.12440. HIV Med. 2016. PMID: 27714978 Review.
-
A systematic review of the genetic mechanisms of dolutegravir resistance.J Antimicrob Chemother. 2019 Nov 1;74(11):3135-3149. doi: 10.1093/jac/dkz256. J Antimicrob Chemother. 2019. PMID: 31280314 Free PMC article.
Cited by
-
Antiretroviral Drugs for Treatment and Prevention of HIV Infection in Adults: 2018 Recommendations of the International Antiviral Society-USA Panel.JAMA. 2018 Jul 24;320(4):379-396. doi: 10.1001/jama.2018.8431. JAMA. 2018. PMID: 30043070 Free PMC article.
-
Cost-effectiveness of pretreatment HIV drug resistance testing in people living with HIV in Iran.PLoS One. 2024 Sep 6;19(9):e0309528. doi: 10.1371/journal.pone.0309528. eCollection 2024. PLoS One. 2024. PMID: 39240944 Free PMC article.
-
Transmitted drug resistance and subtype patterns of viruses from reported new HIV diagnoses in Germany, 2017-2020.BMC Infect Dis. 2023 Oct 10;23(1):673. doi: 10.1186/s12879-023-08649-3. BMC Infect Dis. 2023. PMID: 37817087 Free PMC article.
-
Characterizing HIV-1 Genetic Subtypes and Drug Resistance Mutations among Children, Adolescents and Pregnant Women in Sierra Leone.Genes (Basel). 2021 Aug 26;12(9):1314. doi: 10.3390/genes12091314. Genes (Basel). 2021. PMID: 34573296 Free PMC article.
-
Emergence of Integrase Resistance Mutations During Initial Therapy Containing Dolutegravir.Clin Infect Dis. 2018 Aug 16;67(5):791-794. doi: 10.1093/cid/ciy228. Clin Infect Dis. 2018. PMID: 29933437 Free PMC article.
References
-
- Panel on Antiretroviral Guidelines for Adults and Adolescents. Guidelines for the use of antiretroviral agents in HIV-1 infected adults and adolescents Available at: https://aidsinfo.nih.gov/contentfiles/lvguidelines/adultandadolescentgl.pdf. Accessed 29 March 2017.
-
- European AIDS Clinical Society. Guidelines, version 8.2, 2017 Available at: http://www.eacsociety.org/files/guidelines_8.2-english.pdf. Accessed 29 March 2017.
-
- Hirsch MS, Günthard HF, Schapiro JM et al. ; International AIDS Society-USA Antiretroviral drug resistance testing in adult HIV-1 infection: 2008 recommendations of an International AIDS Society-USA panel. Top HIV Med 2008; 16:266–85. - PubMed
-
- Young B, Fransen S, Greenberg KS et al. . Transmission of integrase strand-transfer inhibitor multidrug-resistant HIV-1: case report and response to raltegravir-containing antiretroviral therapy. Antivir Ther 2011; 16:253–6. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
