

Efficacy and Safety of Degludec versus Glargine in Type 2 Diabetes
- PMID: 28605603
- PMCID: PMC5731244
- DOI: 10.1056/NEJMoa1615692
Efficacy and Safety of Degludec versus Glargine in Type 2 Diabetes
Abstract
Background: Degludec is an ultralong-acting, once-daily basal insulin that is approved for use in adults, adolescents, and children with diabetes. Previous open-label studies have shown lower day-to-day variability in the glucose-lowering effect and lower rates of hypoglycemia among patients who received degludec than among those who received basal insulin glargine. However, data are lacking on the cardiovascular safety of degludec.
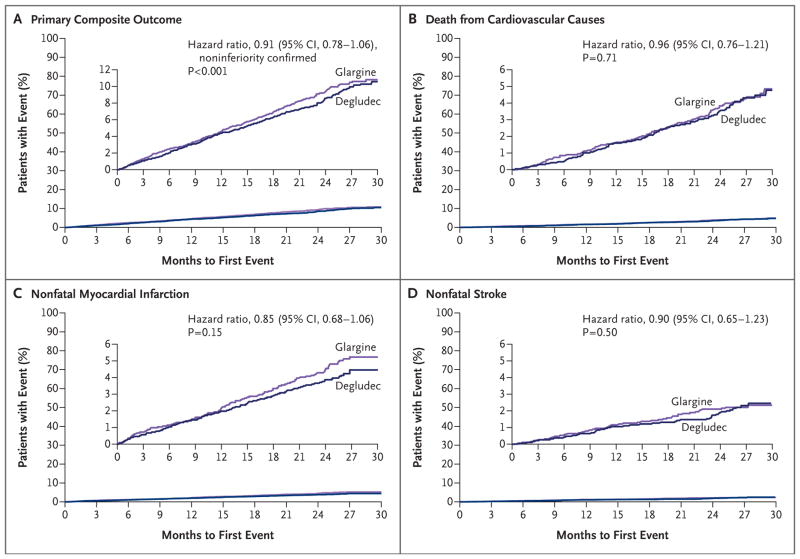
Methods: We randomly assigned 7637 patients with type 2 diabetes to receive either insulin degludec (3818 patients) or insulin glargine U100 (3819 patients) once daily between dinner and bedtime in a double-blind, treat-to-target, event-driven cardiovascular outcomes trial. The primary composite outcome in the time-to-event analysis was the first occurrence of an adjudicated major cardiovascular event (death from cardiovascular causes, nonfatal myocardial infarction, or nonfatal stroke) with a prespecified noninferiority margin of 1.3. Adjudicated severe hypoglycemia, as defined by the American Diabetes Association, was the prespecified, multiplicity-adjusted secondary outcome.
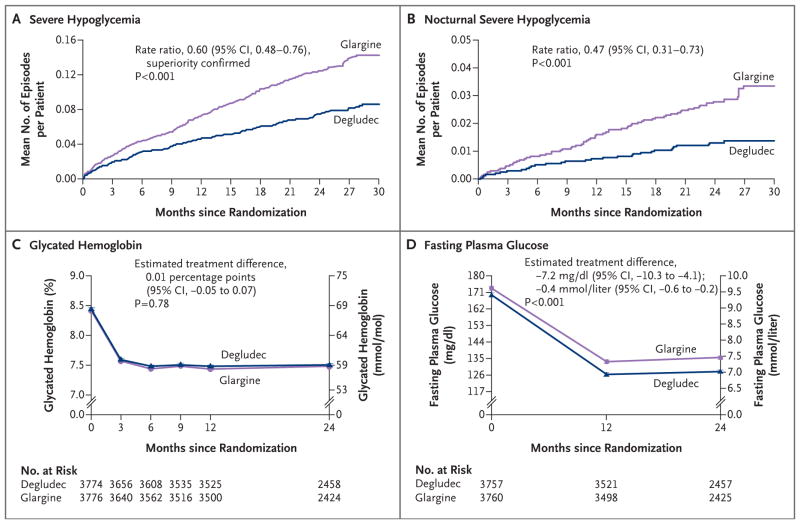
Results: Of the patients who underwent randomization, 6509 (85.2%) had established cardiovascular disease, chronic kidney disease, or both. At baseline, the mean age was 65.0 years, the mean duration of diabetes was 16.4 years, and the mean (±SD) glycated hemoglobin level was 8.4±1.7%; 83.9% of the patients were receiving insulin. The primary outcome occurred in 325 patients (8.5%) in the degludec group and in 356 (9.3%) in the glargine group (hazard ratio, 0.91; 95% confidence interval, 0.78 to 1.06; P<0.001 for noninferiority). At 24 months, the mean glycated hemoglobin level was 7.5±1.2% in each group, whereas the mean fasting plasma glucose level was significantly lower in the degludec group than in the glargine group (128±56 vs. 136±57 mg per deciliter, P<0.001). Prespecified adjudicated severe hypoglycemia occurred in 187 patients (4.9%) in the degludec group and in 252 (6.6%) in the glargine group, for an absolute difference of 1.7 percentage points (rate ratio, 0.60; P<0.001 for superiority; odds ratio, 0.73; P<0.001 for superiority). Rates of adverse events did not differ between the two groups.
Conclusions: Among patients with type 2 diabetes at high risk for cardiovascular events, degludec was noninferior to glargine with respect to the incidence of major cardiovascular events. (Funded by Novo Nordisk and others; DEVOTE ClinicalTrials.gov number, NCT01959529 .).
Figures
Comment in
-
Safety of Degludec versus Glargine in Type 2 Diabetes.N Engl J Med. 2017 Nov 16;377(20):1994. doi: 10.1056/NEJMc1712575. N Engl J Med. 2017. PMID: 29143513 No abstract available.
-
Safety of Degludec versus Glargine in Type 2 Diabetes.N Engl J Med. 2017 Nov 16;377(20):1994-5. doi: 10.1056/NEJMc1712575. N Engl J Med. 2017. PMID: 29143514 No abstract available.
-
Safety of Degludec versus Glargine in Type 2 Diabetes.N Engl J Med. 2017 Nov 16;377(20):1995. doi: 10.1056/NEJMc1712575. N Engl J Med. 2017. PMID: 29143515 No abstract available.
References
-
- Dailey G. Overall mortality in diabetes mellitus: where do we stand today? Diabetes Technol Ther. 2011;13(Suppl 1):S65–S74. - PubMed
-
- Li J, Tong Y, Zhang Y, et al. Effects on all-cause mortality and cardiovascular outcomes in patients with type 2 diabetes by comparing insulin with oral hypoglycemic agent therapy: a meta-analysis of randomized controlled trials. Clin Ther. 2016;38(2):372–386. e6. - PubMed
-
- The ORIGIN Trial Investigators. Basal insulin and cardiovascular and other outcomes in dysglycemia. N Engl J Med. 2012;367:319–28. - PubMed
-
- Tresiba prescribing information. 2015 ( http://www.accessdata.fda.gov/drugsatfda_docs/label/2015/203314lbl.pdf)
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical