

Neurocognitive function in HIV-infected persons with asymptomatic cryptococcal antigenemia: a comparison of three prospective cohorts
- PMID: 28606065
- PMCID: PMC5469183
- DOI: 10.1186/s12883-017-0878-2
Neurocognitive function in HIV-infected persons with asymptomatic cryptococcal antigenemia: a comparison of three prospective cohorts
Abstract
Background: HIV-infected persons with detectable cryptococcal antigen (CrAg) in blood have increased morbidity and mortality compared with HIV-infected persons who are CrAg-negative. This study examined neurocognitive function among persons with asymptomatic cryptococcal antigenemia.
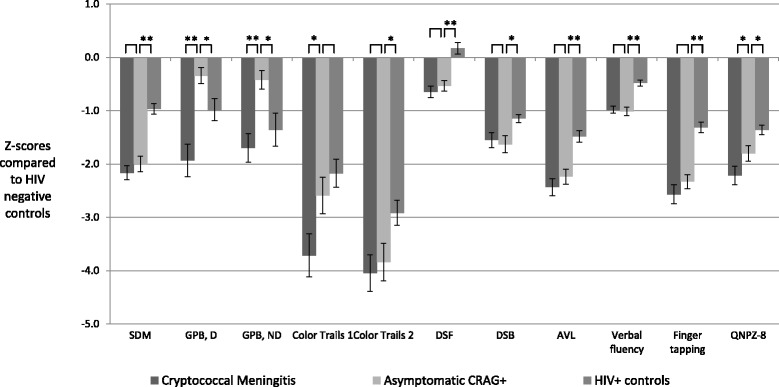
Methods: Participants from three prospective HIV cohorts underwent neurocognitive testing at the time of antiretroviral therapy (ART) initiation. Cohorts included persons with cryptococcal meningitis (N = 90), asymptomatic CrAg + (N = 87), and HIV-infected persons without central nervous system infection (N = 125). Z-scores for each neurocognitive test were calculated relative to an HIV-negative Ugandan population with a composite quantitative neurocognitive performance Z-score (QNPZ-8) created from eight tested domains. Neurocognitive function was measured pre-ART for all three cohorts and additionally after 4 weeks of ART (and 6 weeks of pre-emptive fluconazole) treatment among asymptomatic CrAg + participants.
Results: Cryptococcal meningitis and asymptomatic CrAg + participants had lower median CD4 counts (17 and 26 cells/μL, respectively) than the HIV-infected control cohort (233 cells/μL) as well as lower Karnofsky performance status (60 and 70 vs. 90, respectively). The composite QNPZ-8 for asymptomatic CrAg + (-1.80 Z-score) fell between the cryptococcal meningitis cohort (-2.22 Z-score, P = 0.02) and HIV-infected controls (-1.36, P = 0.003). After four weeks of ART and six weeks of fluconazole, the asymptomatic CrAg + cohort neurocognitive performance improved (-1.0 Z-score, P < 0.001).
Conclusion: Significant deficits in neurocognitive function were identified in asymptomatic CrAg + persons with advanced HIV/AIDS even without signs or sequelae of meningitis. Neurocognitive function in this group improves over time after initiation of pre-emptive fluconazole treatment and ART, but short term adherence support may be necessary.
Keywords: AIDS dementia complex; Cryptococcal meningitis; Cryptococcus; HIV; Neurocognitive disorders; Neuropsychological tests.
Figures
References
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
