

Acute cerebellitis in children: an eleven year retrospective multicentric study in Italy
- PMID: 28606112
- PMCID: PMC5469162
- DOI: 10.1186/s13052-017-0370-z
Acute cerebellitis in children: an eleven year retrospective multicentric study in Italy
Abstract
Background: Acute cerebellitis (AC) and acute cerebellar ataxia (ACA) are the principal causes of acute cerebellar dysfunction in childhood. Nevertheless. there is no accepted consensus regarding the best management of children with AC/ACA: the aim of the study is both to assess clinical, neuroimaging and electrophysiologic features of children with AC/ACA and to evaluate the correlation between clinical parameters, therapy and outcome.
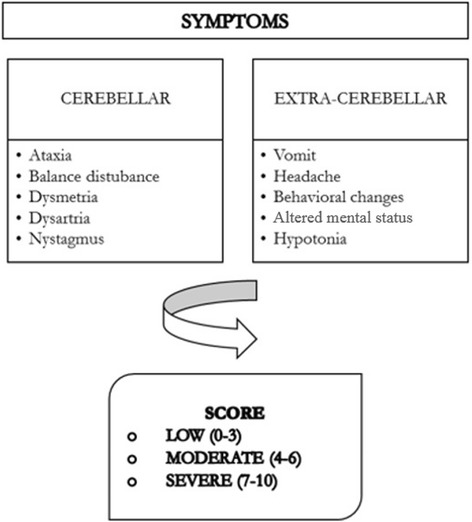
Methods: A multicentric retrospective study was conducted on children ≤ 18 years old admitted to 12 Italian paediatric hospitals for AC/ACA from 01/01/2003 to 31/12/2013. A score based on both cerebellar and extracerebellar signs/symptoms was computed for each patient. One point was given for each sign/symptom reported. Severity was divided in three classes: low, moderate, severe.
Results: A total of 124 children were included in the study. Of these, 118 children received a final diagnosis of ACA and 6 of AC. The most characteristic finding of AC/ACA was a broad-based gait disturbance. Other common symptoms included balance disturbances, slurred speech, vomiting, headache and fever. Neurological sequelae were reported in 6 cases (5%) There was no correlation among symptoms, cerebrospinal fluid findings, clinical outcome. There was no correlation between clinical manifestations and clinical score on admission and length of hospital stay, sex, age and EEG findings with sequelae (P > 0.05). Children with pathological magnetic resonance imaging (MRI) or computed tomography (CT) had a higher probability of having clinical sequelae. Treatment was decided independently case by case. Patients with a higher clinical score on admission had a higher probability of receiving intravenous steroids.
Conclusions: We confirmed the literature data about the benign course of AC/ACA in most cases but we also highlighted a considerable rate of patients with neurological sequelae (5%). Pathological MRI or CT findings at admission correlate to neurological sequelae. These findings suggest the indication to perform an instrumental evaluation in all patients with AC/ACA at admission to identify those at higher risk of neurological outcome. These patients may benefit from a more aggressive therapeutic strategy and should have a closer follow-up. Randomized controlled trials are needed to confirm these observations. The ultimate goal of these studies could be to develop a standardized protocol on AC/ACA. The MRI/CT data, associated with the clinical manifestations, may allow us to define the class risk of patients for a neurological outcome.
Keywords: Cerebellitis; Children; Outcome; Therapy.
Figures
References
-
- Amador N, Scheithauer BW, Giannini C, Raffel C. Acute cerebellitis presenting as tumor. Report of two cases. J Neurosurg 2007; 107(1)(Suppl)57–61. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
