

Outcomes of cement beads and cement spacers in the treatment of bone defects associated with post-traumatic osteomyelitis
- PMID: 28606128
- PMCID: PMC5468979
- DOI: 10.1186/s12891-017-1614-1
Outcomes of cement beads and cement spacers in the treatment of bone defects associated with post-traumatic osteomyelitis
Abstract
Background: Cement spacers (Masquelet technique) have traditionally been used for the treatment of segmental bone defects. However, no reports have used cement spacers for the treatment of small/partial segmental bone defects associated with osteomyelitis and compared the outcomes with cement beads.
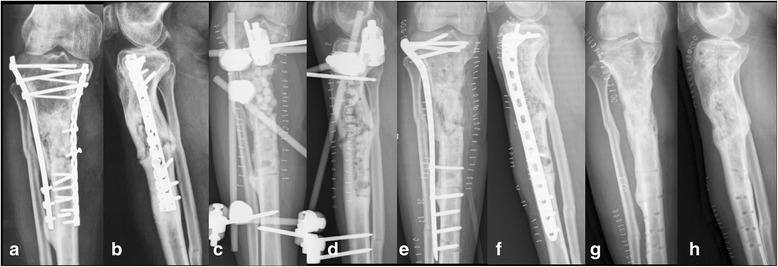
Methods: We retrospectively analysed 40 patients with post-traumatic osteomyelitis of the tibia who underwent treatment, which was performed in two stages. In the first stage, thorough debridement was performed, and bone defects were filled with either antibiotic-impregnated cement beads (bead group, 18 patients) or spacers (spacer group, 22 patients). In the second stage, the cement beads or spacers were removed (for the spacer group, the induced membrane formed by the spacer was preserved) and the bone defects were filled with cancellous autografts.
Results: All patients in the bead group had small/partial segmental bone defects after debridement, while 3 patients in the spacer group had large/segmental bone defects. The mean volume of bone defects of the spacer group (40.4 cm3) was significantly larger than that of the bead group (32.4 cm3). The infection control rate (88.9%,16/18 vs 90.9%, 20/22), bone healing time (8.5 months vs 7.5 months) and complication rates (22.2%, 4/18 vs 27.2%, 6/22) were comparable between bead group and spacer group.
Conclusion: The results of this study suggest that cement spacers may have an infection control rate comparable to cement beads in the treatment of bone defects associated with post-traumatic osteomyelitis. Furthermore, cement spacers could be used for the reconstruction of small/partial segmental bone defects as well as for large/segmental bone defects, whereas cement beads were not suitable for the reconstruction of large/segmental bone defects.
Keywords: Bone defect; Cement bead; Cement spacer; Masquelet technique; Osteomyelitis.
Figures

References
-
- Juutilainen V. Posttraumatic osteomyelitis. Suomen Ortopedia ja Traumatologia. 2011;34(1):38–41.
-
- Cabanela ME. Open cancellous bone grafting of infected bone defects. Orthop Clin North Am. 1984;15(3):427–440. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
