

Drivers of expenditure on primary care prescription drugs in 10 high-income countries with universal health coverage
- PMID: 28606975
- PMCID: PMC5468103
- DOI: 10.1503/cmaj.161481
Drivers of expenditure on primary care prescription drugs in 10 high-income countries with universal health coverage
Abstract
Background: Managing expenditures on pharmaceuticals is important for health systems to sustain universal access to necessary medicines. We sought to estimate the size and sources of differences in expenditures on primary care medications among high-income countries with universal health care systems.
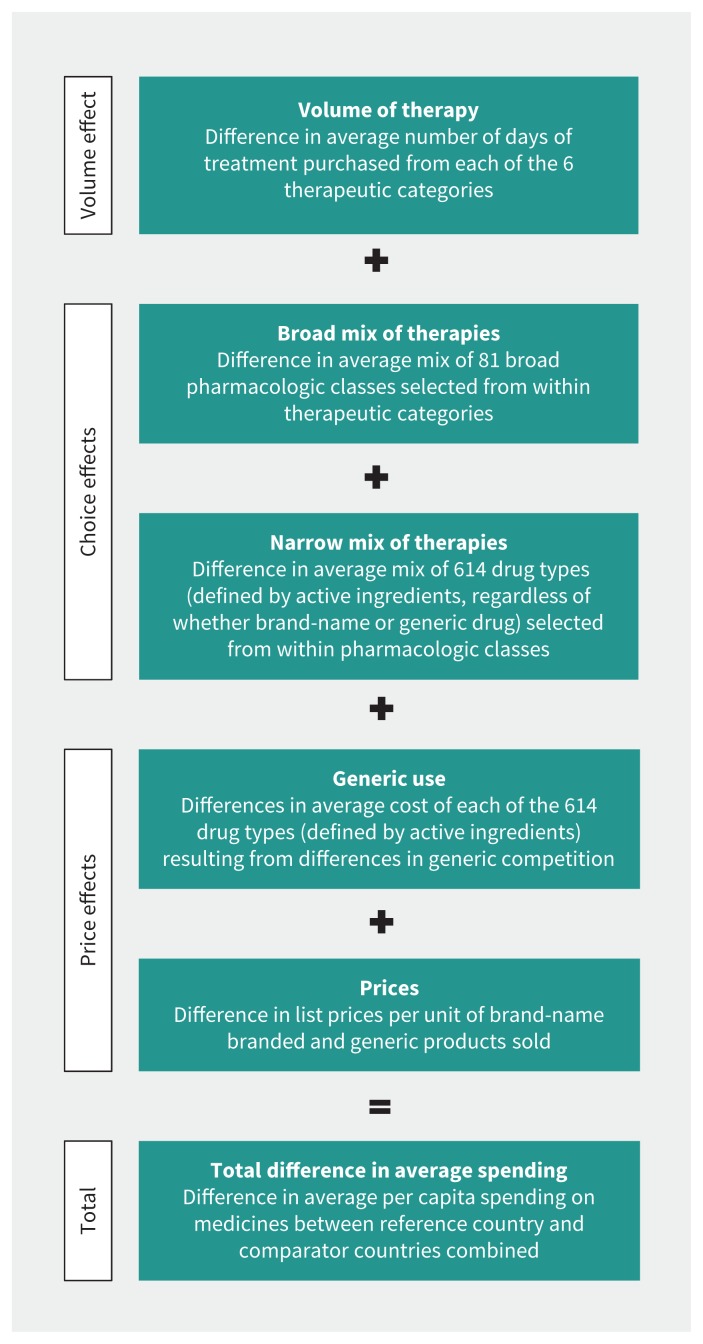
Methods: We compared data on the 2015 volume and cost per day of primary care prescription drug therapies purchased in 10 high-income countries with various systems of universal health care coverage (7 from Europe, in addition to Australia, Canada and New Zealand). We measured total per capita expenditure on 6 categories of primary care prescription drugs: hypertension treatments, pain medications, lipid-lowering medicines, noninsulin diabetes treatments, gastrointestinal preparations and antidepressants. We quantified the contributions of 5 drivers of the observed differences in per capita expenditures.
Results: Across countries, the average annual per capita expenditure on the primary care medicines studied varied by more than 600%: from $23 in New Zealand to $171 in Switzerland. The volume of therapies purchased varied by 41%: from 198 days per capita in Norway to 279 days per capita in Germany. Most of the differences in average expenditures per capita were driven by a combination of differences in the average mix of drugs selected within therapeutic categories and differences in the prices paid for medicines prescribed.
Interpretation: Significant international differences in average expenditures on primary care medications are driven primarily by factors that contribute to the average daily cost of therapy, rather than differences in the volume of therapy used. Average expenditures were lower among single-payer financing systems that appeared to promote lower prices and the selection of lower-cost treatment options.
© 2017 Canadian Medical Association or its licensors.
Conflict of interest statement
Competing interests: None declared.
Figures
Comment in
-
Drug prices: How do we get to a better place?CMAJ. 2017 Jun 12;189(23):E792-E793. doi: 10.1503/cmaj.170440. CMAJ. 2017. PMID: 28606974 Free PMC article. No abstract available.
References
-
- OECD health statistics 2016. Paris: Organisation for Economic Co-operation and Development; 2016.
-
- Global medicines use in 2020 — outlook and implications. Parsippany (NJ): IMS Health; 2015.
-
- Osborn R, Moulds D, Squires D, et al. International survey of older adults finds shortcomings in access, coordination, and patient-centered care. New York: The Commonwealth Fund; 2014. - PubMed
-
- Patented Medicine Prices Review Board: annual report 2014. Ottawa: Patented Medicine Prices Review Board; 2015.
-
- Barnes S, Anderson L. Low earnings, unfilled prescriptions: employer-provided health benefit coverage in Canada. Toronto: Wellesley Institute; 2015.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources