

Pharmacokinetics of Pyrazinamide and Optimal Dosing Regimens for Drug-Sensitive and -Resistant Tuberculosis
- PMID: 28607022
- PMCID: PMC5527644
- DOI: 10.1128/AAC.00490-17
Pharmacokinetics of Pyrazinamide and Optimal Dosing Regimens for Drug-Sensitive and -Resistant Tuberculosis
Abstract
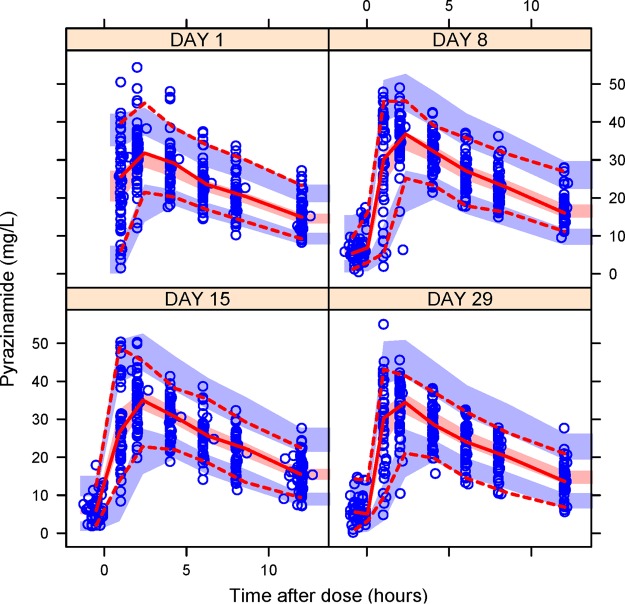
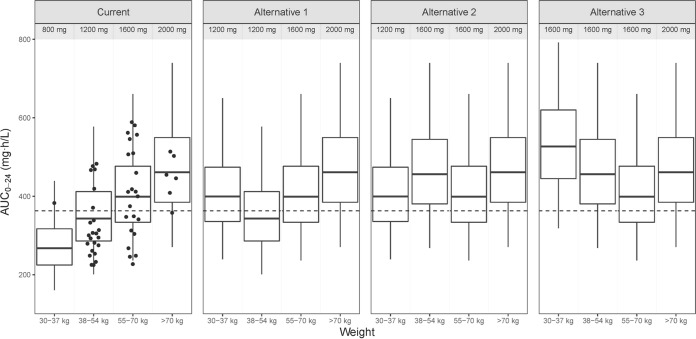
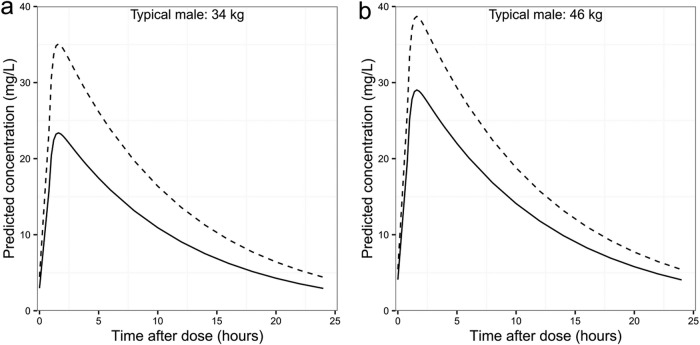
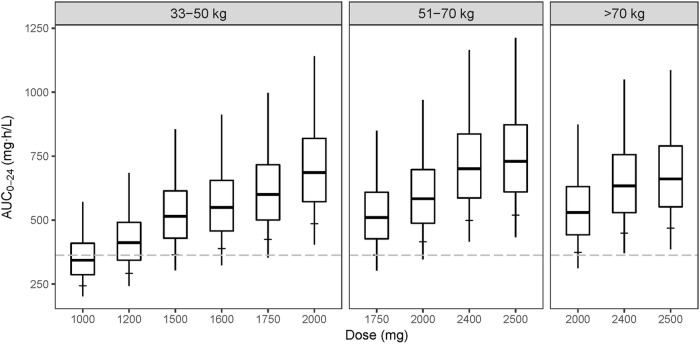
Pyrazinamide is used in the treatment of tuberculosis (TB) because its sterilizing effect against tubercle bacilli allows the shortening of treatment. It is part of standard treatment for drug-susceptible and drug-resistant TB, and it is being considered as a companion drug in novel regimens. The aim of this analysis was to characterize factors contributing to the variability in exposure and to evaluate drug exposures using alternative doses, thus providing evidence to support revised dosing recommendations for drug-susceptible and multidrug-resistant tuberculosis (MDR-TB). Pyrazinamide pharmacokinetic (PK) data from 61 HIV/TB-coinfected patients in South Africa were used in the analysis. The patients were administered weight-adjusted doses of pyrazinamide, rifampin, isoniazid, and ethambutol in fixed-dose combination tablets according to WHO guidelines and underwent intensive PK sampling on days 1, 8, 15, and 29. The data were interpreted using nonlinear mixed-effects modeling. PK profiles were best described using a one-compartment model with first-order elimination. Allometric scaling was applied to disposition parameters using fat-free mass. Clearance increased by 14% from the 1st day to the 29th day of treatment. More than 50% of patients with weight less than 55 kg achieved lower pyrazinamide exposures at steady state than the targeted area under the concentration-time curve from 0 to 24 h of 363 mg · h/liter. Among patients with drug-susceptible TB, adding 400 mg to the dose for those weighing 30 to 54 kg improved exposure. Average pyrazinamide exposure in different weight bands among patients with MDR-TB could be matched by administering 1,500 mg, 1,750 mg, and 2,000 mg to patients in the 33- to 50-kg, 51- to 70-kg, and greater than 70-kg weight bands, respectively.
Keywords: AUC; HIV/TB coinfection; NONMEM; fat-free mass; population pharmacokinetics; weight band dosing.
Copyright © 2017 American Society for Microbiology.
Figures
References
-
- Konno K, Feldmann FM, McDermott W. 1967. Pyrazinamide susceptibility and amidase activity of tubercle bacilli. Am Rev Respir Dis 95:461–469. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
