

Intraoperative assessment of tumor margins during glioma resection by desorption electrospray ionization-mass spectrometry
- PMID: 28607048
- PMCID: PMC5495278
- DOI: 10.1073/pnas.1706459114
Intraoperative assessment of tumor margins during glioma resection by desorption electrospray ionization-mass spectrometry
Abstract
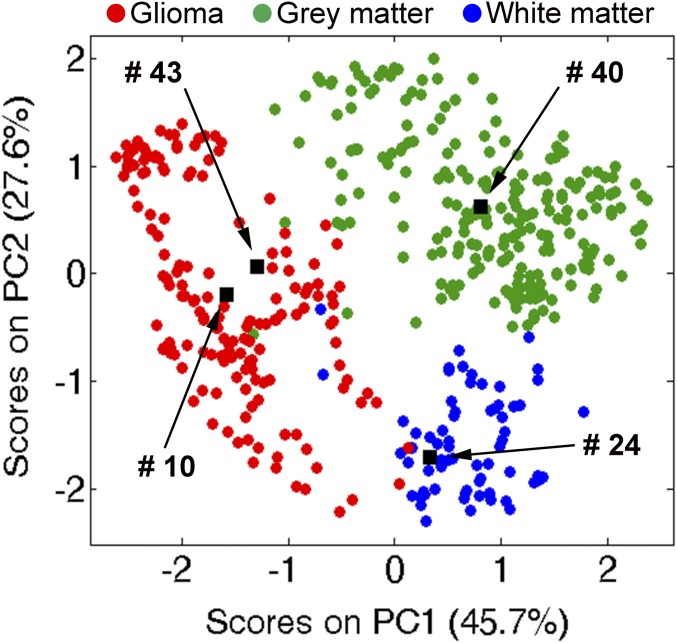
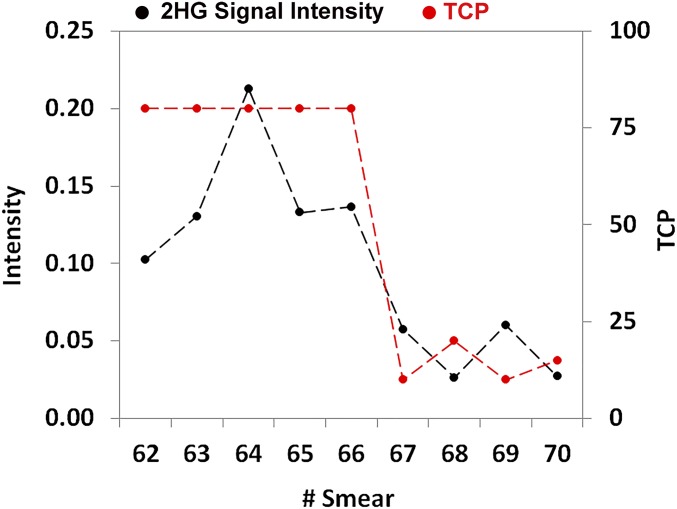
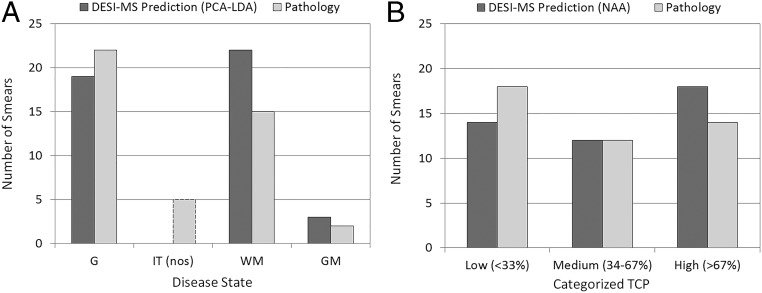
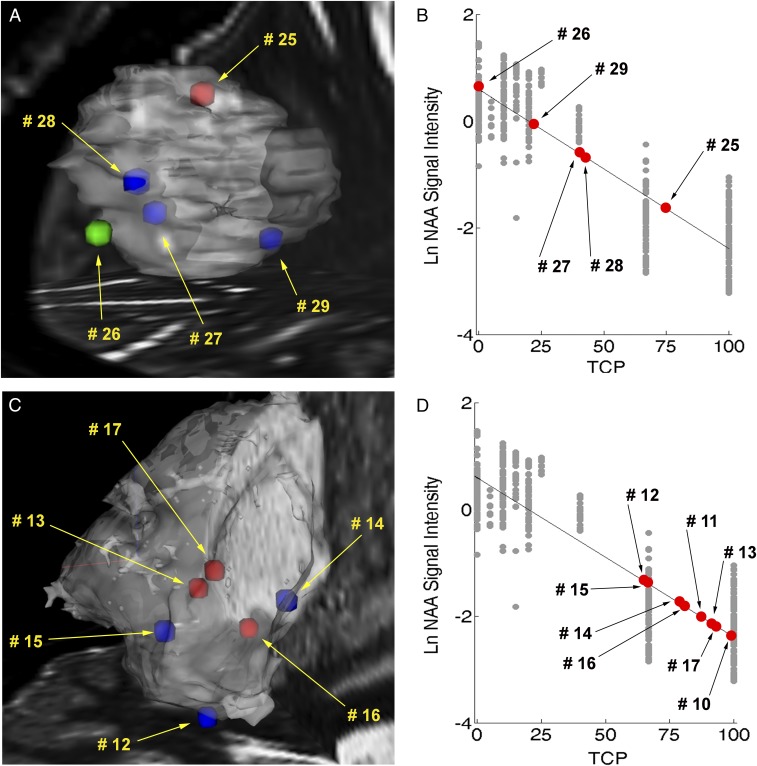
Intraoperative desorption electrospray ionization-mass spectrometry (DESI-MS) is used to characterize tissue smears by comparison with a library of DESI mass spectra of pathologically determined tissue types. Measurements are performed in the operating room within 3 min. These mass spectra provide direct information on tumor infiltration into white or gray brain matter based on N-acetylaspartate (NAA) and on membrane-derived complex lipids. The mass spectra also indicate the isocitrate dehydrogenase mutation status of the tumor via detection of 2-hydroxyglutarate, currently assessed postoperatively on biopsied tissue using immunohistochemistry. Intraoperative DESI-MS measurements made at surgeon-defined positions enable assessment of relevant disease state of tissue within the tumor mass and examination of the resection cavity walls for residual tumor. Results for 73 biopsies from 10 surgical resection cases show that DESI-MS allows detection of glioma and estimation of high tumor cell percentage (TCP) at surgical margins with 93% sensitivity and 83% specificity. TCP measurements from NAA are corroborated by indirect measurements based on lipid profiles. Notably, high percentages (>50%) of unresected tumor were found in one-half of the margin biopsy smears, even in cases where postoperative MRI suggested gross total tumor resection. Unresected tumor causes recurrence and malignant progression, as observed within a year in one case examined in this study. These results corroborate the utility of DESI-MS in assessing surgical margins for maximal safe tumor resection. Intraoperative DESI-MS analysis of tissue smears, ex vivo, can be inserted into the current surgical workflow with no alterations. The data underscore the complexity of glioma infiltration.
Keywords: ambient ionization; glioma; lipids; neurological smears; tumor infiltration.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Orringer D, et al. Extent of resection in patients with glioblastoma: Limiting factors, perception of resectability, and effect on survival. J Neurosurg. 2012;117:851–859. - PubMed
-
- Hervey-Jumper SL, Berger MS. Maximizing safe resection of low- and high-grade glioma. J Neurooncol. 2016;130:269–282. - PubMed
-
- Louis DN, et al. The 2016 World Health Organization Classification of Tumors of the Central Nervous System: A summary. Acta Neuropathol. 2016;131:803–820. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
