

Anatomical dilatation of the superior vena cava associated with an arrhythmogenic response induced by SVC scan pacing after atrial fibrillation ablation
- PMID: 28607612
- PMCID: PMC5459421
- DOI: 10.1016/j.joa.2016.10.003
Anatomical dilatation of the superior vena cava associated with an arrhythmogenic response induced by SVC scan pacing after atrial fibrillation ablation
Abstract
Background: The relationship between pulmonary vein (PV) arrhythmogenicity and its anatomy has been reported. However, that of the superior vena cava (SVC) has not been well discussed. Arrhythmogenic response induced by pacing stimulation at SVC might help with identifying SVC arrhythmogenicity. The purpose of this study was to investigate the relationship between the anatomical dilatation of SVC and the arrhythmogenic response induced by pacing at SVC.
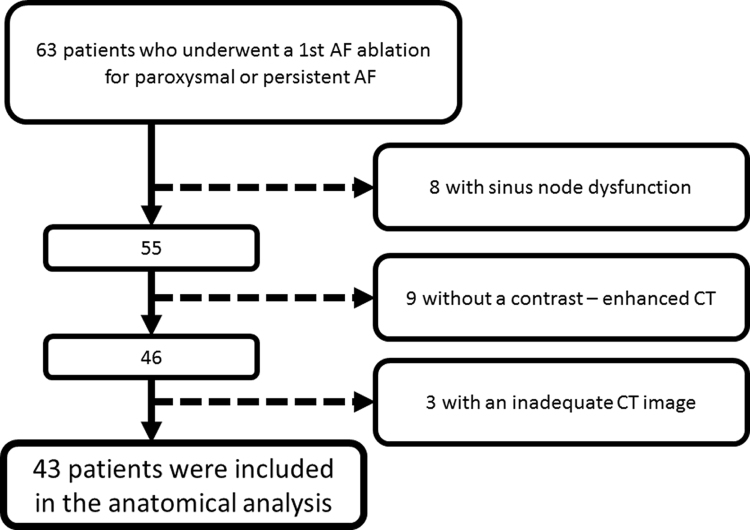
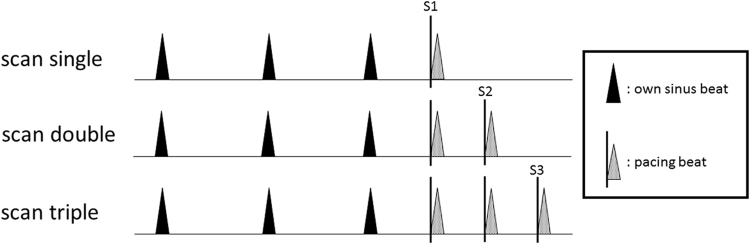
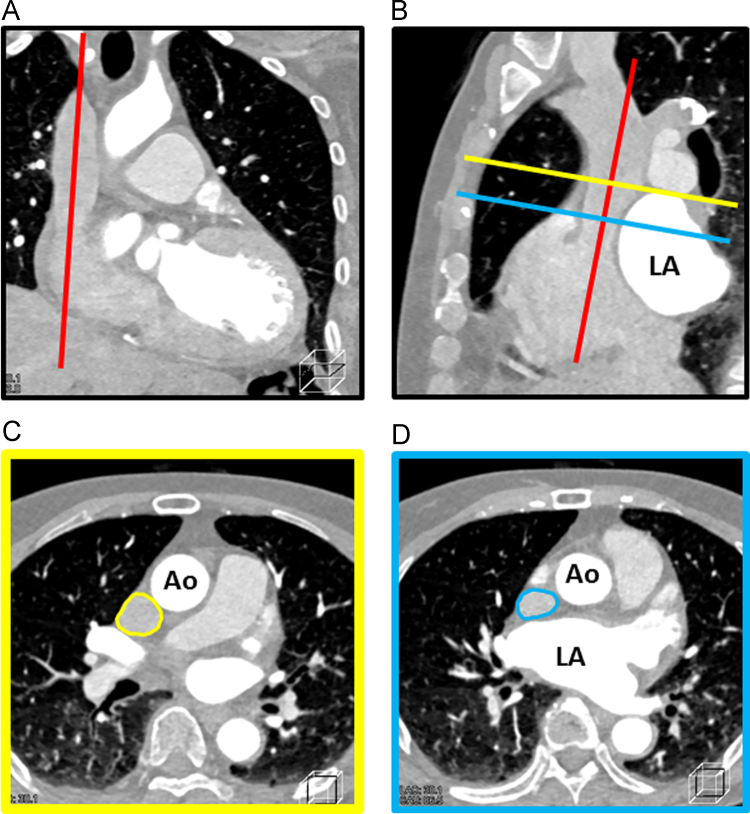
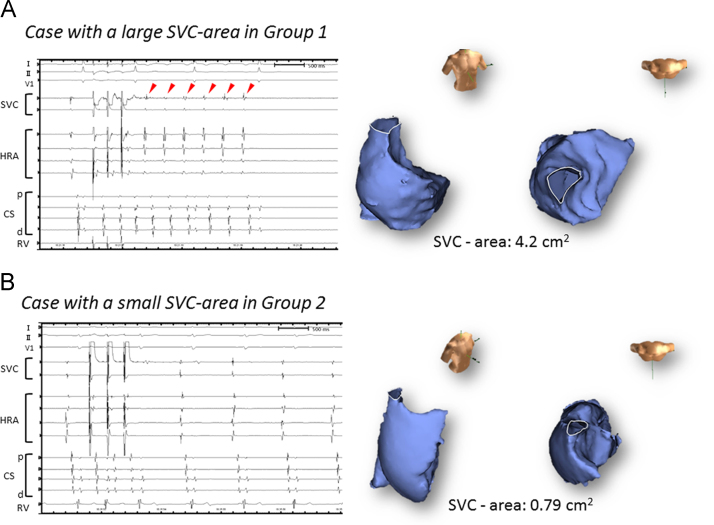
Methods: Forty-three patients who underwent atrial fibrillation (AF) ablation were enrolled in this study. After PV isolation, scan pacing (up to triple extra stimulation following intrinsic sinus beats) was performed at SVC. The arrhythmogenic response was defined as following: (1) repetitive atrial responses, (2) non-sustained, and (3) sustained AF/ atrial tachycardia. To assess the dilatation of SVC, we measured the cross-sectional area of the SVC (SVC-area) using multi-planar reconstruction CT imaging.
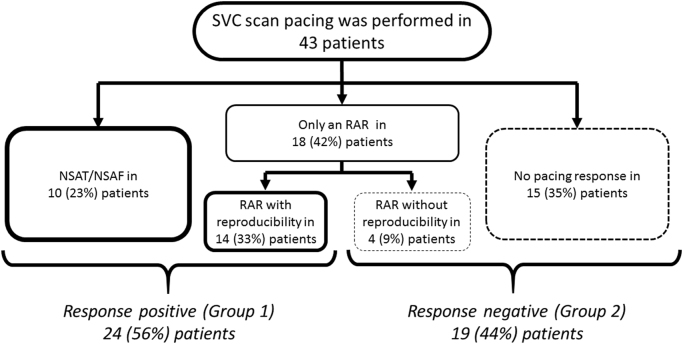
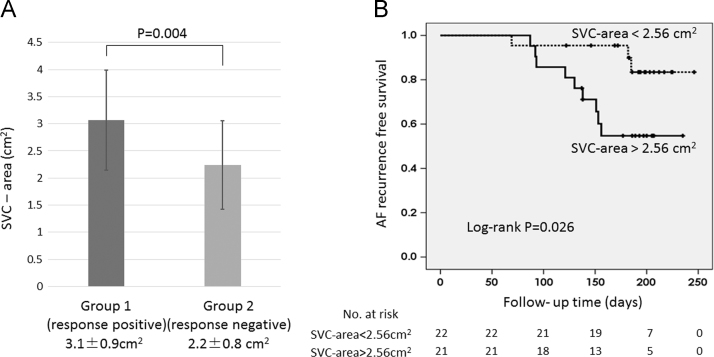
Results: Arrhythmogenic responses were documented in 24 patients (Group 1). No arrhythmogenic responses were documented in the remaining 19 patients (Group 2). The SVC-area was significantly larger in Group 1 than Group 2 (3.1±0.9 vs. 2.2±0.8 cm2, P=0.004). A multivariate analysis revealed only SVC-area was associated with arrhythmogenic responses (odds ratio=2.87, CI 1.05-7.82, P=0.04). Furthermore, AF recurrence rate was significantly higher in patients with SVC-area>2.56 cm2 than those with SVC-area <2.56 cm2 (9 [42.9%] of 21 vs. 3 [13.6%] of 22, P=0.026).
Conclusion: Dilatation of SVC was associated with an arrhythmogenic response, and the AF recurrence rate was significantly higher in patients with large SVC-area. Adjunctive catheter intervention for the SVC might be indicated in patients with a dilated SVC and an arrhythmogenic response.
Keywords: AF, atrial fibrillation; AT, atrial tachycardia; Arrhythmogenic response; Atrial fibrillation; CT, computed tomography; Catheter ablation; PV, pulmonary vein; SVC, superior vena cava; Scan pacing; Superior vena cava.
Figures
References
-
- Haissaguerre M., Jais P., Shah D.C. Spontaneous initiation of atrial fibrillation by ectopic beats originating in the pulmonary veins. N Engl J Med. 1998;339:659–666. - PubMed
-
- Liu X., Dong J., Mavrakis H.E. Achievement of pulmonary vein isolation in patients undergoing circumferential pulmonary vein ablation: a randomized comparison between two different isolation approaches. J Cardiovasc Electrophysiol. 2006;17:1263–1270. - PubMed
-
- Packer D.L., Kowal R.C., Wheelan K.R. Cryoballoon ablation of pulmonary veins for paroxysmal atrial fibrillation: first results of the North American Arctic Front (STOP AF) pivotal trial. J Am Coll Cardiol. 2013;61:1713–1723. - PubMed
-
- Lin W.S., Tai C.T., Hsieh M.H. Catheter ablation of paroxysmal atrial fibrillation initiated by non-pulmonary vein ectopy. Circulation. 2003;107:3176–3183. - PubMed
-
- Shah D., Haissaguerre M., Jais P., Hocini M. Nonpulmonary vein foci: do they exist? Pacing Clin Electrophysiol. 2003;26:1631–1635. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
