

Complex fractionated atrial electrograms, high dominant frequency regions, and left atrial voltages during sinus rhythm and atrial fibrillation
- PMID: 28607613
- PMCID: PMC5459411
- DOI: 10.1016/j.joa.2016.10.001
Complex fractionated atrial electrograms, high dominant frequency regions, and left atrial voltages during sinus rhythm and atrial fibrillation
Abstract
Background: Ablation targeting complex fractionated atrial electrograms (CFAEs) or high dominant frequency (DF) sites is generally effective for persistent atrial fibrillation (AF). CFAEs and/or high DF sites may exist in low-voltage regions, which theoretically represent abnormal substrates. However, whether CFAEs or high DF sites reflect low voltage substrates during sinus rhythm (SR) is unknown.
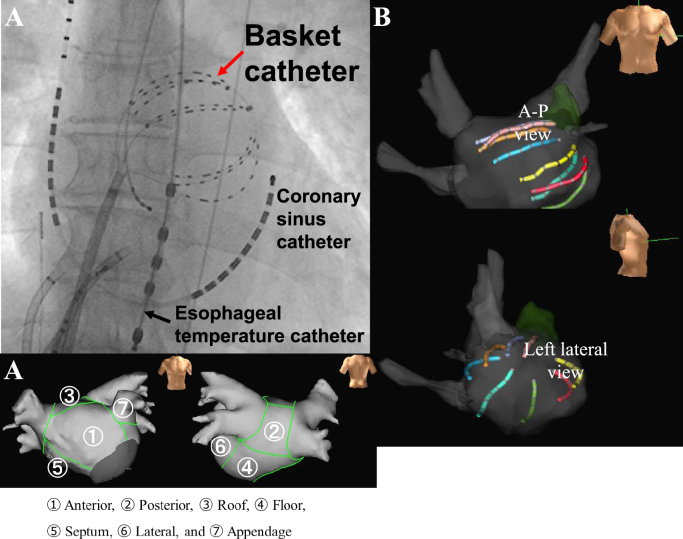
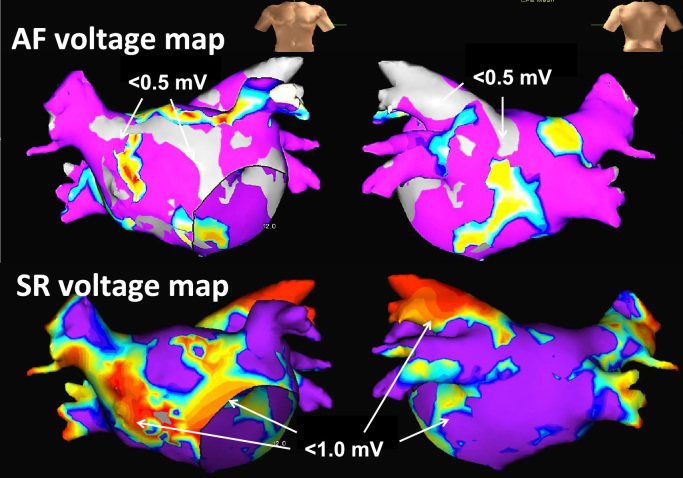
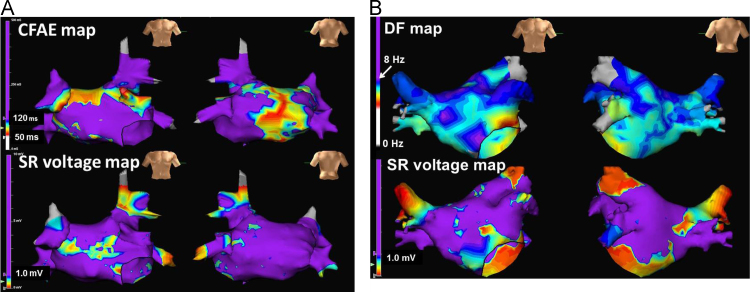
Methods: Sixteen patients with AF (8 with paroxysmal AF; 8, persistent AF) underwent high-density mapping of the left atrium (LA) with a 3-dimensional electroanatomic mapping system before ablation. The LA was divided into 7 segments and the mean bipolar voltage recorded during AF and SR, CFAEs (cycle lengths of 50-120 ms), and DF sites were assessed in each segment with either a duo-decapolar ring catheter (n=10) or a 64-pole basket catheter (n=6). Low-voltage areas were defined as those of <0.5 mV during AF and <1.0 mV during SR.
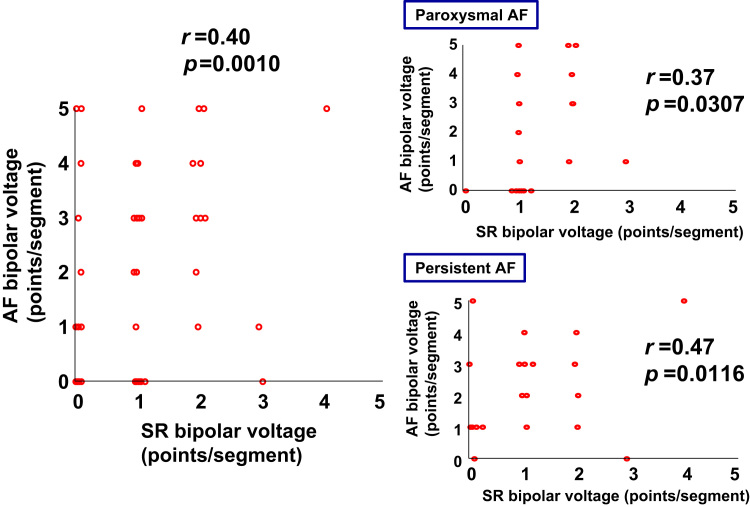
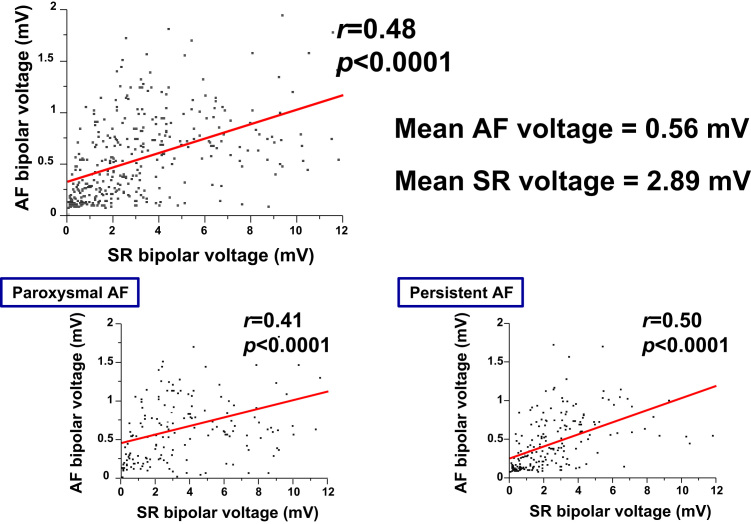
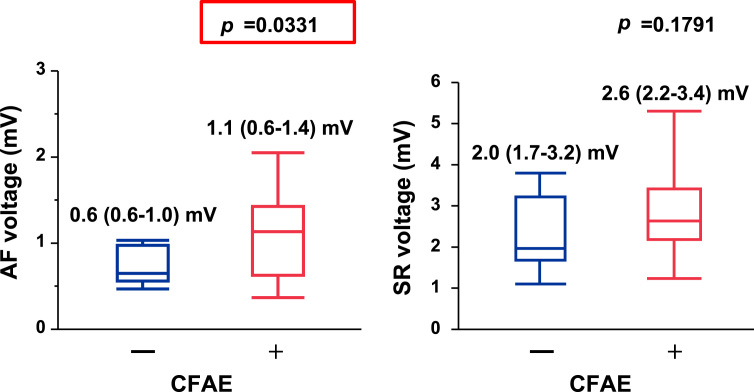
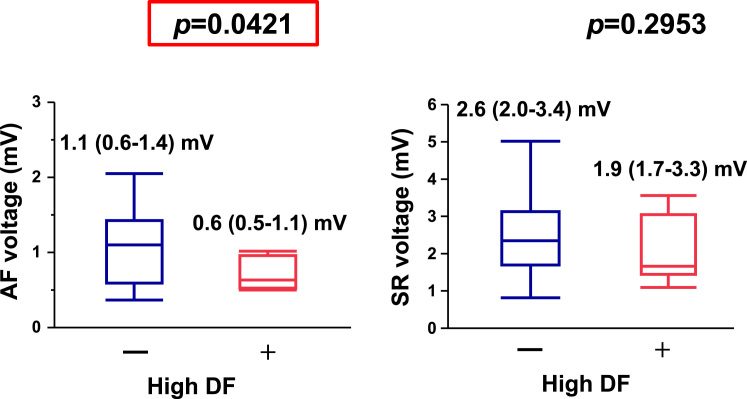
Results: Regional mean voltage recorded from the basket catheter showed good correlation between AF and SR (r=0.60, p<0.01); however, the % low-voltage area in the LA recorded from the ring catheter showed weak correlation (r=0.34, p=0.05). Mean voltage was lower during AF than during SR (1.0 mV [IQR, 0.5-1.4] vs. 2.6 mV [IQR, 1.8-3.6], p<0.01). The regional and overall % low-voltage area of the LA was greater during AF than during SR (20% vs. 11%, p=0.05). CFAEs and high DF sites (>8 Hz) did not correlate with % low-voltage sites during SR; however, CFAEs sites were located in high-voltage regions during AF and high DF sites were located in low voltage regions during AF.
Conclusions: CFAEs and high DF areas during AF do not reflect damaged atrial myocardium as shown by the SR voltage. However, CFAEs and high DF sites may demonstrate different electrophysiologic properties because of different voltage amplitude during AF.
Keywords: Atrial fibrillation; Complex fractionated atrial electrogram; Dominant frequency; Sinus rhythm.
Figures
Similar articles
-
Localized rotational activation in the left atrium during human atrial fibrillation: relationship to complex fractionated atrial electrograms and low-voltage zones.Heart Rhythm. 2013 Dec;10(12):1830-8. doi: 10.1016/j.hrthm.2013.09.007. Epub 2013 Sep 7. Heart Rhythm. 2013. PMID: 24016695
-
Comparative distribution of complex fractionated atrial electrograms, high dominant frequency (HDF) sites during atrial fibrillation and HDF sites during sinus rhythm.J Interv Card Electrophysiol. 2013 Apr;36(3):297-306. doi: 10.1007/s10840-012-9748-4. Epub 2012 Nov 20. J Interv Card Electrophysiol. 2013. PMID: 23179918 Clinical Trial.
-
Spatial and temporal variability of the complex fractionated atrial electrogram activity and dominant frequency in human atrial fibrillation.J Arrhythm. 2015 Apr;31(2):101-7. doi: 10.1016/j.joa.2014.08.004. Epub 2014 Sep 26. J Arrhythm. 2015. PMID: 26336540 Free PMC article.
-
The optimal automatic algorithm for the mapping of complex fractionated atrial electrograms in patients with atrial fibrillation.J Cardiovasc Electrophysiol. 2010 Jan;21(1):21-6. doi: 10.1111/j.1540-8167.2009.01567.x. J Cardiovasc Electrophysiol. 2010. PMID: 19656247
-
Validating left atrial fractionation and low-voltage substrate during atrial fibrillation and sinus rhythm-A high-density mapping study in persistent atrial fibrillation.Front Cardiovasc Med. 2022 Oct 18;9:1000027. doi: 10.3389/fcvm.2022.1000027. eCollection 2022. Front Cardiovasc Med. 2022. PMID: 36330001 Free PMC article.
Cited by
-
Entropy Mapping Approach for Functional Reentry Detection in Atrial Fibrillation: An In-Silico Study.Entropy (Basel). 2019 Feb 18;21(2):194. doi: 10.3390/e21020194. Entropy (Basel). 2019. PMID: 33266909 Free PMC article.
-
Left atrial voltage mapping: defining and targeting the atrial fibrillation substrate.J Interv Card Electrophysiol. 2019 Dec;56(3):213-227. doi: 10.1007/s10840-019-00537-8. Epub 2019 May 10. J Interv Card Electrophysiol. 2019. PMID: 31076965 Free PMC article. Review.
-
Wavefront direction and cycle length affect left atrial electrogram amplitude.J Arrhythm. 2017 Aug;33(4):269-274. doi: 10.1016/j.joa.2017.01.001. Epub 2017 Feb 13. J Arrhythm. 2017. PMID: 28765756 Free PMC article.
-
Clinical and Structural Factors Affecting Ablation Outcomes in Atrial Fibrillation Patients - A Review.Curr Cardiol Rev. 2023;19(5):83-96. doi: 10.2174/1573403X19666230331103153. Curr Cardiol Rev. 2023. PMID: 36999694 Free PMC article. Review.
References
-
- Wazni O., Wilkoff B., Saliba W. Catheter ablation for atrial fibrillation. N Engl J Med. 2011;365:2296–2304. - PubMed
-
- Nademanee K., McKenzie J., Kosar E. A new approach for catheter ablation of atrial fibrillation: mapping of electrophysiologic substrate. J Am Coll Cardiol. 2004;43:2044–2053. - PubMed
-
- Haïssaguerre M., Sanders P., Hocini M. Catheter ablation of long-lasting persistent atrial fibrillation: critical structures for termination. J Cardiovasc Electrophysiol. 2005;16:1125–1137. - PubMed
-
- O׳Neill M.D., Jaïs P., Takahashi Y. The stepwise ablation approach for chronic atrial fibrillation--evidence for a cumulative effect. J Interv Card Electrophysiol. 2006;16:153–167. - PubMed
-
- Schmitt C., Estner H., Hecher B. Radiofrequency ablation of complex fractionated atrial electrograms (CFAE): preferential sites of acute termination and regularization in paroxysmal and persistent atrial fibrillation. J Cardiovasc Electrophysiol. 2007;18:1039–1046. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
