

A proposal of clinical ECG index "vagal score" for determining the mechanism of paroxysmal atrioventricular block
- PMID: 28607616
- PMCID: PMC5459424
- DOI: 10.1016/j.joa.2016.10.004
A proposal of clinical ECG index "vagal score" for determining the mechanism of paroxysmal atrioventricular block
Abstract
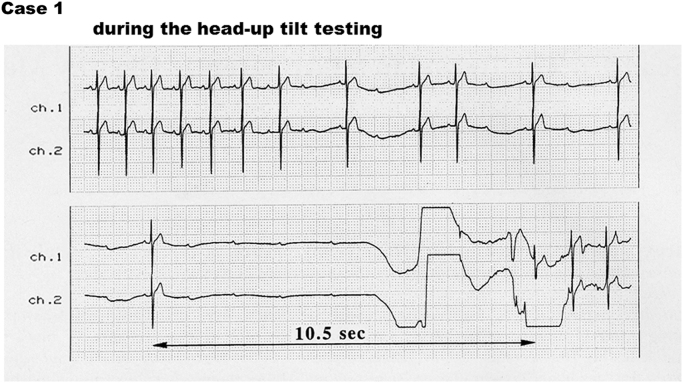
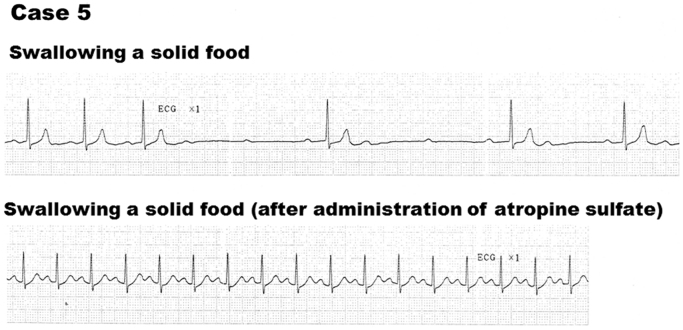
Background: Paroxysmal atrioventricular block (P-AVB) is a well-known cause of syncope; however, its underlying mechanism is difficult to determine. This study aimed to evaluate a new ECG index, the "vagal score (VS)," to determine the mechanism of P-AVB.
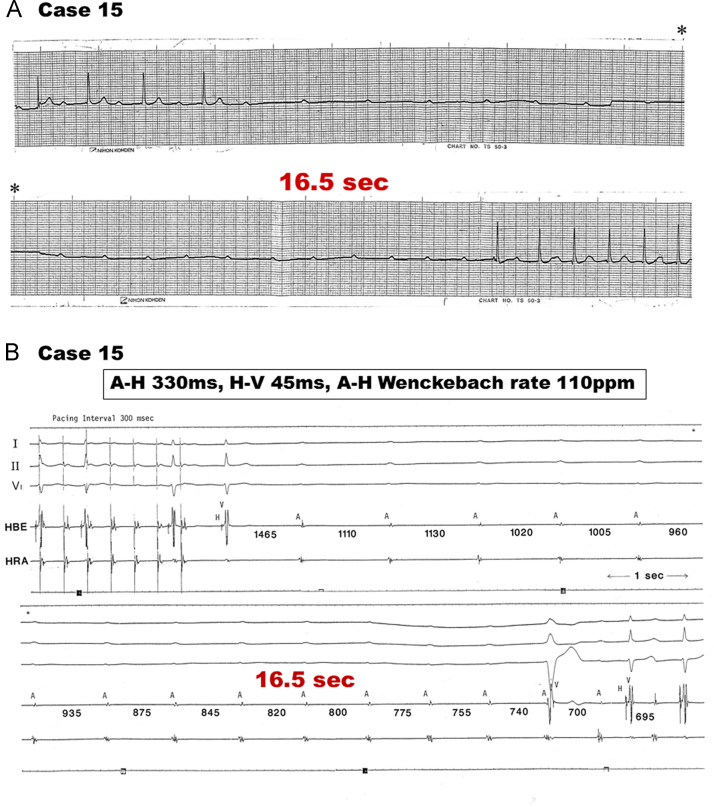
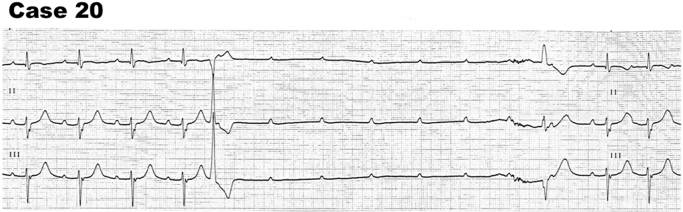
Methods: We evaluated the VS in 20 patients with P-AVB (13 men, 7 women; aged 25-78 years [mean, 59.3 years]). The VS was developed by assigning 1 point each for the following: (1) no AVB or intraventricular conduction disturbance on the baseline ECG, (2) PR prolongation immediately before P-AVB, (3) sinus slowing immediately before P-AVB, (4) initiation of P-AVB by PP prolongation, (5) sinus slowing during ventricular asystole, and (6) resumption of AV conduction with PP shortening, and by assigning -1 point each for (7) the initiation of P-AVB by a premature beat, and (8) resumption of AV conduction by an escape beat. Based on the clinical situations and electrophysiologic findings, we considered the mechanism of P-AVB as vagally mediated or intrinsic conduction disease (ICD).
Results: The VS ranged from 5 to -2 points for each patient. Five patients with a definite vagally mediated P-AVB had high VSs (3-5 points). We observed characteristic ECG findings of ICD consisting of changes in AV conduction by an extrasystole and/or escape beat in only 5 of the 6 patients (83%) with a low VS (1 to -2).
Conclusions: The VS is simple and potentially useful for determining the mechanism of P-AVB. P-AVB with a VS ≥3 strongly suggested a vagally mediated mechanism.
Keywords: Electrocardiogram (ECG); Intrinsic conduction disease; Mechanism; Paroxysmal atrioventricular block; Vagally mediated.
Figures
Similar articles
-
Five cases of complete atrioventricular block induced by bending forward: unusual but not unique.Europace. 2021 Sep 8;23(9):1487-1492. doi: 10.1093/europace/euab044. Europace. 2021. PMID: 33693701
-
Etiology of syncope in patients with preexisting atrioventricular conduction disorders.Pacing Clin Electrophysiol. 2020 Nov;43(11):1268-1272. doi: 10.1111/pace.14064. Epub 2020 Sep 22. Pacing Clin Electrophysiol. 2020. PMID: 32901951
-
Benefits of fetal echocardiographic surveillance in pregnancies at risk of congenital heart block: single-center study of 212 anti-Ro52-positive pregnancies.Ultrasound Obstet Gynecol. 2019 Jul;54(1):87-95. doi: 10.1002/uog.20214. Epub 2019 Jun 7. Ultrasound Obstet Gynecol. 2019. PMID: 30620419
-
Mobitz type II second-degree atrioventricular block: a commonly overdiagnosed and misinterpreted arrhythmia.Front Cardiovasc Med. 2024 Aug 29;11:1450705. doi: 10.3389/fcvm.2024.1450705. eCollection 2024. Front Cardiovasc Med. 2024. PMID: 39267806 Free PMC article. Review.
-
Syncope and paroxysmal atrioventricular block.J Arrhythm. 2017 Dec;33(6):562-567. doi: 10.1016/j.joa.2017.03.008. Epub 2017 May 8. J Arrhythm. 2017. PMID: 29255501 Free PMC article. Review.
Cited by
-
A case of paroxysmal atrioventricular block with atrial pacemaker shift during ventricular arrest.J Arrhythm. 2020 Aug 2;36(5):950-951. doi: 10.1002/joa3.12417. eCollection 2020 Oct. J Arrhythm. 2020. PMID: 33024478 Free PMC article.
-
Clinical Efficacy of Catheter Ablation in the Treatment of Vasovagal Syncope.J Clin Med. 2022 Sep 13;11(18):5371. doi: 10.3390/jcm11185371. J Clin Med. 2022. PMID: 36143017 Free PMC article.
-
Perservative paroxysmal atrioventricular block : Cardiac syncope misdiagnosed as anxiety for more than 20 years.Herzschrittmacherther Elektrophysiol. 2017 Sep;28(3):335-339. doi: 10.1007/s00399-017-0528-9. Herzschrittmacherther Elektrophysiol. 2017. PMID: 28840364 English.
-
A case of advanced atrioventricular block after gynecological surgery.JA Clin Rep. 2020 Oct 9;6(1):81. doi: 10.1186/s40981-020-00387-8. JA Clin Rep. 2020. PMID: 33034755 Free PMC article. No abstract available.
-
Case report of paroxysmal atrioventricular block and ventricular arrest in a young pregnant woman: What is the mechanism?Ann Noninvasive Electrocardiol. 2022 Mar;27(2):e12909. doi: 10.1111/anec.12909. Epub 2021 Oct 28. Ann Noninvasive Electrocardiol. 2022. PMID: 34708449 Free PMC article.
References
-
- Lee S., Wellens H.J.J., Josephson M.E. Paroxysmal atrioventricular block. Heart Rhythm. 2009;6:1229–1234. - PubMed
-
- Alboni P., Holz A., Brignole M. Vagally mediated atrioventricular block: pathophysiology and diagnosis. Heart. 2013;99:904–908. - PubMed
-
- Sumiyoshi M., Nakata Y., Mineda Y. Paroxysmal atrioventricular block induced during head-up tilt testing in an apparently healthy man. J Cardiovasc Electrophysiol. 1997;8:561–564. - PubMed
-
- Rosenbaum M.B., Elizare M.V., Levi R.J. Paroxysmal atrioventricular block related to hypopolarization and spontaneous diastolic depolarization. Chest. 1973;63:678–688. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
