

A Multifaceted Quality Improvement Programme to Improve Acute Kidney Injury Care and Outcomes in a Large Teaching Hospital
- PMID: 28607684
- PMCID: PMC5457974
- DOI: 10.1136/bmjquality.u219176.w7476
A Multifaceted Quality Improvement Programme to Improve Acute Kidney Injury Care and Outcomes in a Large Teaching Hospital
Abstract
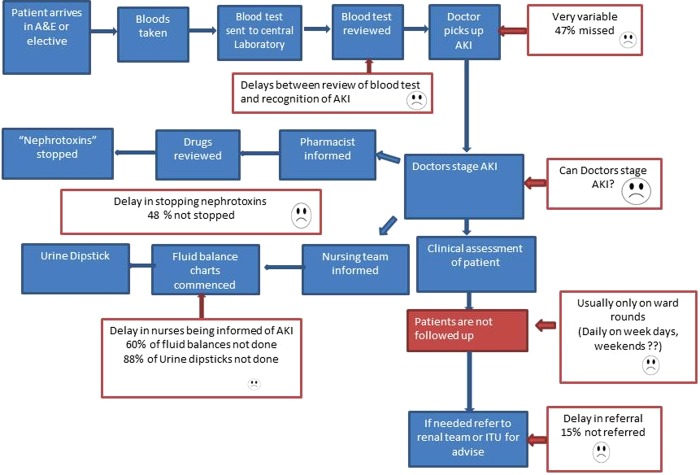
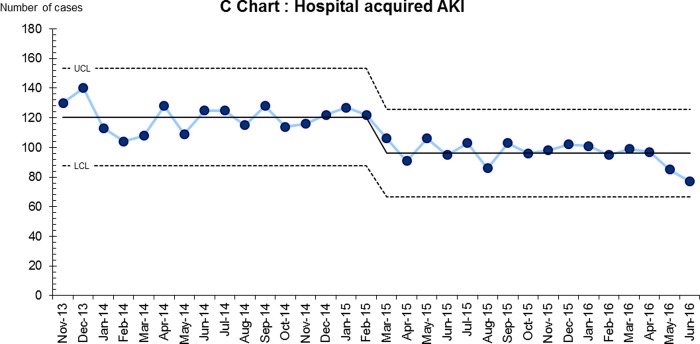
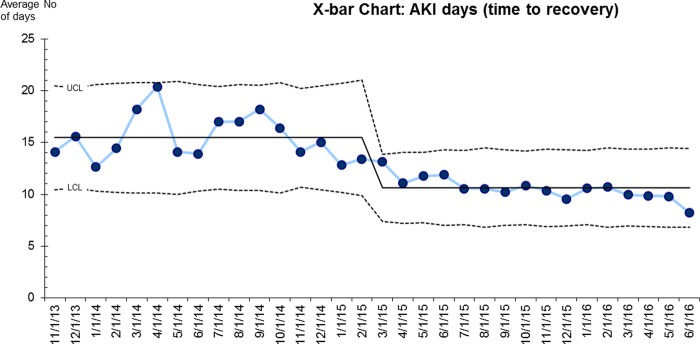
Acute kidney injury (AKI) is now widely recognised as a serious health care issue, occurring in up to 25% of hospital in-patients, often with worsening of outcomes. There have been several reports of substandard care in AKI. This quality improvement (QI) programme aimed to improve AKI care and outcomes in a large teaching hospital. Areas of documented poor AKI care were identified and specific improvement activities implemented through sequential Plan-Do-Study-Act (PDSA) cycles. An electronic alert system (e-alert) for AKI was developed, a Priority Care Checklist (PCC) was tested with the aid of specialist nurses whilst targeted education activities were carried out and data on care processes and outcomes monitored. The e-alert had a sensitivity of 99% for the detection of new cases of AKI. Key aspects of the PCC saw significant improvements in their attainment: Detection of AKI within 24 hours from 53% to 100%, fluid assessment from 42% to 90%, drug review 48% to 95% and adherence to nine key aspects of care from 40% to 90%. There was a significant reduction in variability of delivered AKI care. AKI incidence reduced from 9% of all hospitalisations at baseline to 6.5% (28% reduction), AKI related length of stay reduced from 22.1 days to 17 days (23% reduction) and time to recovery (AKI days) 15.5 to 9.8 days (36% reduction). AKI related deaths also showed a trend towards reduction, from an average of 38 deaths to 34 (10.5%). The number of cases of hospital acquired AKI were reduced by 28% from 120 to 86 per month. This study demonstrates significant improvements related to a QI programme combining e-alerts, a checklist implemented by a nurse and education in improving key processes of care. This resulted in sustained improvement in key patient outcomes.
Figures
References
-
- Kaufman J, Dhakal M, Patel B et al. Community-acquired acute renal failure. Am J Kidney Dis 1991;17:191–8. - PubMed
-
- Hoste EA, Schurgers M. Epidemiology of acute kidney injury: how big is the problem? Crit Care Med 2008;36:S146–51. - PubMed
-
- Selby NM, Crowley L, Fluck RJ et al. Use of Electronic Results Reporting to Diagnose and Monitor AKI in Hospitalized Patients. Clinical Journal of the American Society of Nephrology 2012;7:533–540. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources