

A Comparative Study of Pharyngeal Repair in Two Layers Versus Three Layers, Following Total Laryngectomy in Carcinoma of Larynx
- PMID: 28607897
- PMCID: PMC5446349
- DOI: 10.1007/s12070-017-1108-3
A Comparative Study of Pharyngeal Repair in Two Layers Versus Three Layers, Following Total Laryngectomy in Carcinoma of Larynx
Abstract
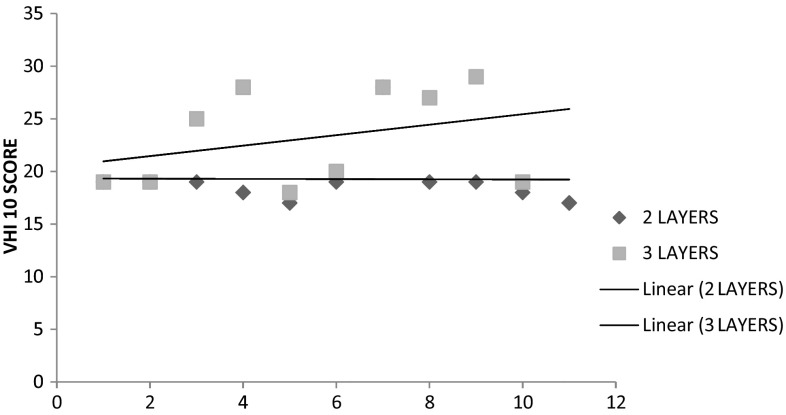
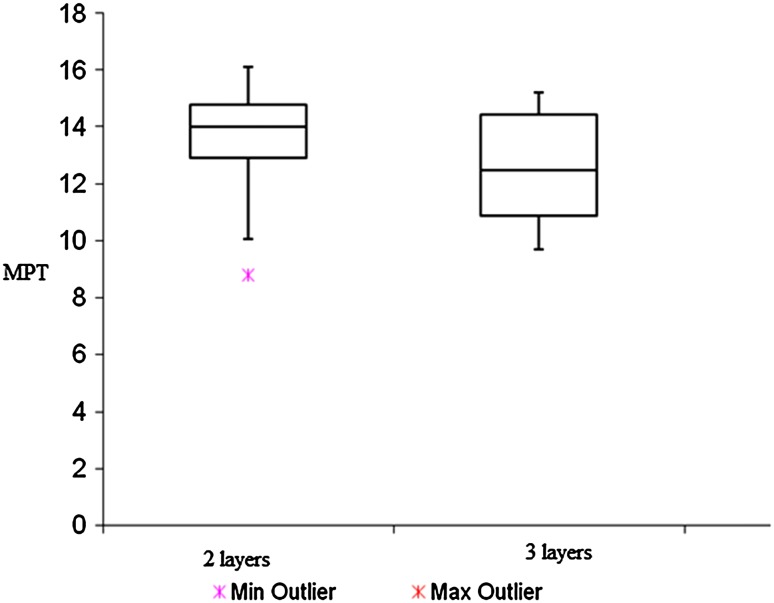
Larynx is the second most common site for cancer in the upper aerodigestive tract. One of the dreaded complications following total laryngectomy has been pharyngo cutaneous fistula (PCF). PCF merits special attention due to its significant negative impact on the recovery process. Total laryngectomy profoundly alters speech. Effective voice restoration is essential for the rehabilitation of these patients. Inadequate consensus exists as to the best technique of pharyngeal repair to decrease incidence of PCF and ensure good quality voice following total laryngectomy. 21 patients were included in the study for total laryngectomy with trachea oesophageal voice prosthesis placement. Patients were randomised into 2 groups. Group A had their pharynx repaired in two layers and Group B had it done in three layers. Post operatively the patients were followed up for a period of 12 months to look for incidence of PCF. Subjective and objective evaluation of voice was done. 9.52% of patients developed PCF. All of the cases of PCF were in the group repaired in three layers. In cases with repair by two layers the mean Voice Handicap Index 10 (VHI 10) score was 19.27 and those with three layers pharyngeal repair was 23.20. Average maximum phonation time amongst the study population was 13.09. In three layers and two layers pharyngeal repair the average maximum phonation time was 12.56 and 13.58 respectively. Surgical repair of pharynx in two layers excluding the third layer of pharyngeal musculature reduces the chance of PCF. Two layers pharyngeal repair supplemented by cricopharyngeal myotomy led to significantly better voice outcome.
Keywords: Laryngeal neoplasms; Laryngectomy; Neoplasm staging; Pharyngectomy; Speech; Suture techniques.
Conflict of interest statement
Conflict of interest
The authors of this article declare that he/she has no conflict of interest.
Human and Animal Rights
Animals were not involved in this study.
Ethical Approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed Consent
Informed consent was obtained from all individual participants included in the study.
Figures
References
-
- Markou K, Vlachtsis K, Nikolaou A, Petridis D, Kouloulas A, Daniilidis I. Incidence and predisposing factors of pharyngocutaneous fistula formation after total laryngectomy. Is there a relationship with tumor recurrence? Eur Arch Otorhinolaryngol. 2004;261(2):61–67. doi: 10.1007/s00405-003-0643-6. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources