

Can proportional ventilation modes facilitate exercise in critically ill patients? A physiological cross-over study : Pressure support versus proportional ventilation during lower limb exercise in ventilated critically ill patients
- PMID: 28608135
- PMCID: PMC5468357
- DOI: 10.1186/s13613-017-0289-y
Can proportional ventilation modes facilitate exercise in critically ill patients? A physiological cross-over study : Pressure support versus proportional ventilation during lower limb exercise in ventilated critically ill patients
Abstract
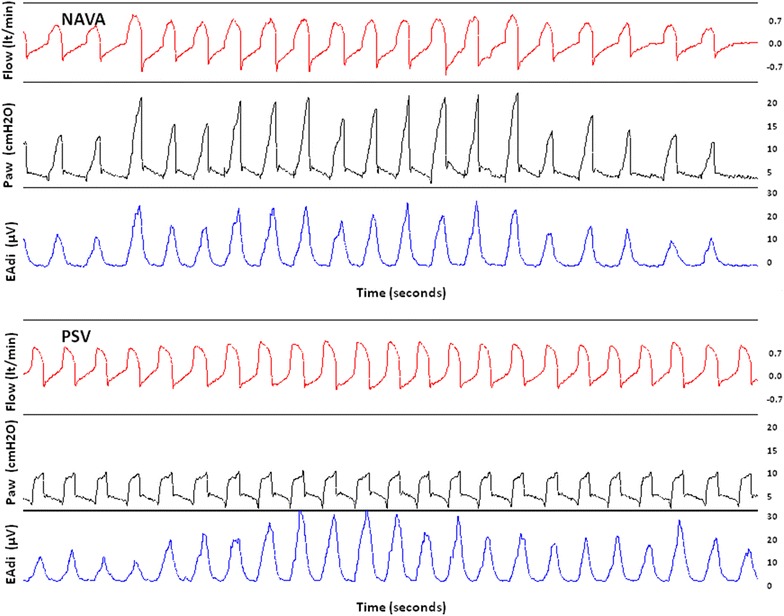
Background: Early exercise of critically ill patients may have beneficial effects on muscle strength, mass and systemic inflammation. During pressure support ventilation (PSV), a mismatch between demand and assist could increase work of breathing and limit exercise. A better exercise tolerance is possible with a proportional mode of ventilation (Proportional Assist Ventilation, PAV+ and Neurally Adjusted Ventilatory Assist, NAVA). We examined whether, in critically ill patients, PSV and proportional ventilation have different effects on respiratory muscles unloading and work efficiency during exercise.
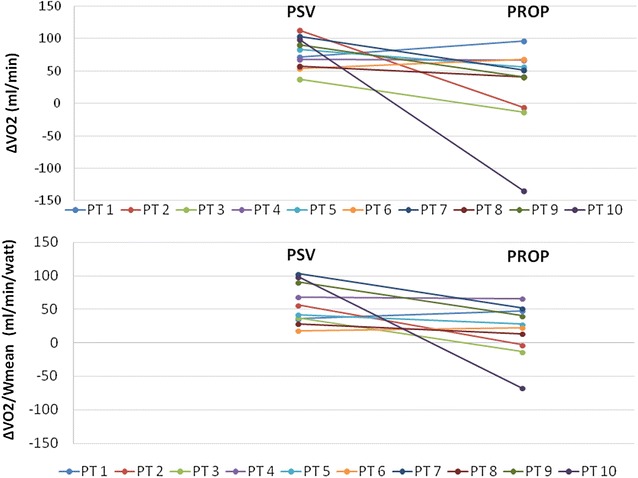
Methods: Prospective pilot randomized cross-over study performed in a medico-surgical ICU. Patients requiring mechanical ventilation >48 h were enrolled. At initiation, the patients underwent an incremental workload test on a cycloergometer to determine the maximum level capacity. The next day, 2 15-min exercise, at 60% of the maximum capacity, were performed while patients were randomly ventilated with PSV and PAV+ or NAVA. The change in oxygen consumption (ΔVO2, indirect calorimetry) and the work efficiency (ratio of ΔVO2 per mean power) were computed.
Results: Ten patients were examined, 6 ventilated with PSV/PAV+ and 4 with PSV/NAVA. Despite the same mean inspiratory pressure at baseline between the modes, baseline VO2 (median, IQR) was higher during proportional ventilation (301 ml/min, 270-342) compared to PSV (249 ml/min, 206-353). Exercise with PSV was associated with a significant increase in VO2 (ΔVO2, median, IQR) (77.6 ml/min, 59.9-96.5), while VO2 did not significantly change during exercise with proportional modes (46.3 ml/min, 5.7-63.7, p < 0.05). As a result, exercise with proportional modes was associated with a better work efficiency than with PSV. The ventilator modes did not affect patient's dyspnea, limb fatigue, distance, hemodynamics and breathing pattern.
Conclusions: Proportional ventilation during exercise results in higher work efficiency and less increase in VO2 compared to ventilation with PSV. These preliminary findings suggest that proportional ventilation could enhance the training effect and facilitate rehabilitation.
Keywords: Assisted mechanical ventilation; Critically ill patients; Exercise; Oxygen consumption; Proportional ventilation; Work efficiency.
Figures

References
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
