

Predicting Infectious ComplicatioNs in Children with Cancer: an external validation study
- PMID: 28609435
- PMCID: PMC5520507
- DOI: 10.1038/bjc.2017.154
Predicting Infectious ComplicatioNs in Children with Cancer: an external validation study
Abstract
Background: The aim of this study was to validate the 'Predicting Infectious ComplicatioNs in Children with Cancer' (PICNICC) clinical decision rule (CDR) that predicts microbiologically documented infection (MDI) in children with cancer and fever and neutropenia (FN). We also investigated costs associated with current FN management strategies in Australia.
Methods: Demographic, episode, outcome and cost data were retrospectively collected on 650 episodes of FN. We assessed the discrimination, calibration, sensitivity and specificity of the PICNICC CDR in our cohort compared with the derivation data set.
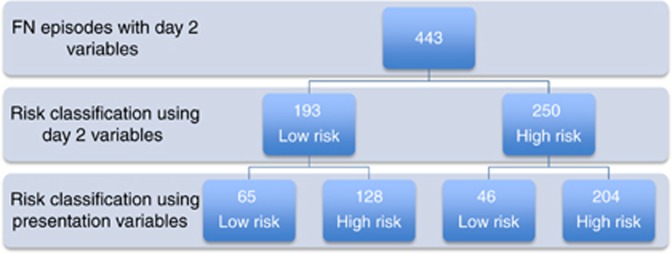
Results: Using the original variable coefficients, the CDR performed poorly. After recalibration the PICNICC CDR had an area under the receiver operating characteristic (AUC-ROC) curve of 0.638 (95% CI 0.590-0.685) and calibration slope of 0.24. The sensitivity, specificity, positive predictive value and negative predictive value of the PICNICC CDR at presentation was 78.4%, 39.8%, 28.6% and 85.7%, respectively. For bacteraemia, the sensitivity improved to 85.2% and AUC-ROC to 0.71. Application at day 2, taking into consideration the proportion of MDI known (43%), further improved the sensitivity to 87.7%. Length of stay is the main contributor to cost of FN treatment, with an average cost per day of AUD 2183 in the low-risk group.
Conclusions: For prediction of any MDI, the PICNICC rule did not perform as well at presentation in our cohort as compared with the derivation study. However, for bacteraemia, the predictive ability was similar to that of the derivation study, highlighting the importance of recalibration using local data. Performance also improved after an overnight period of observation. Implementation of a low-risk pathway, using the PICNICC CDR after a short period of inpatient observation, is likely to be safe and has the potential to reduce health-care expenditure.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Alexander SW, Wade KC, Hibberd PL, Parsons SK (2002) Evaluation of risk prediction criteria for episodes of febrile neutropenia in children with cancer. J Pediatr Hematol Oncol 24(1): 38–42. - PubMed
-
- Altman DG, Royston P (2000) What do we mean by validating a prognostic model? Stat Med 19(4): 453–473. - PubMed
-
- Ammann RA, Bodmer N, Hirt A, Niggli FK, Nadal D, Simon A, Ozsahin H, Kontny U, Kuhne T, Popovic MB, Luthy AR, Aebi C (2010) Predicting adverse events in children with fever and chemotherapy-induced neutropenia: the prospective multicenter SPOG 2003 FN study. J Clin Oncol 28(12): 2008–2014. - PubMed
-
- Ammann RA, Hirt A, Luthy AR, Aebi C (2003) Identification of children presenting with fever in chemotherapy-induced neutropenia at low risk for severe bacterial infection. Med Pediatr Oncol 41(5): 436–443. - PubMed
-
- Baorto EP, Aquino VM, Mullen C, Buchanan GR, DeBaun MR (2001) Clinical parameters associated with low bacteremia risk in 1100 pediatric oncology patients with fever and neutropenia. Cancer 92(4): 909–913. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
