

Effect of Abdominal Ultrasound on Clinical Care, Outcomes, and Resource Use Among Children With Blunt Torso Trauma: A Randomized Clinical Trial
- PMID: 28609532
- PMCID: PMC5815005
- DOI: 10.1001/jama.2017.6322
Effect of Abdominal Ultrasound on Clinical Care, Outcomes, and Resource Use Among Children With Blunt Torso Trauma: A Randomized Clinical Trial
Abstract
Importance: The utility of the focused assessment with sonography for trauma (FAST) examination in children is unknown.
Objective: To determine if the FAST examination during initial evaluation of injured children improves clinical care.
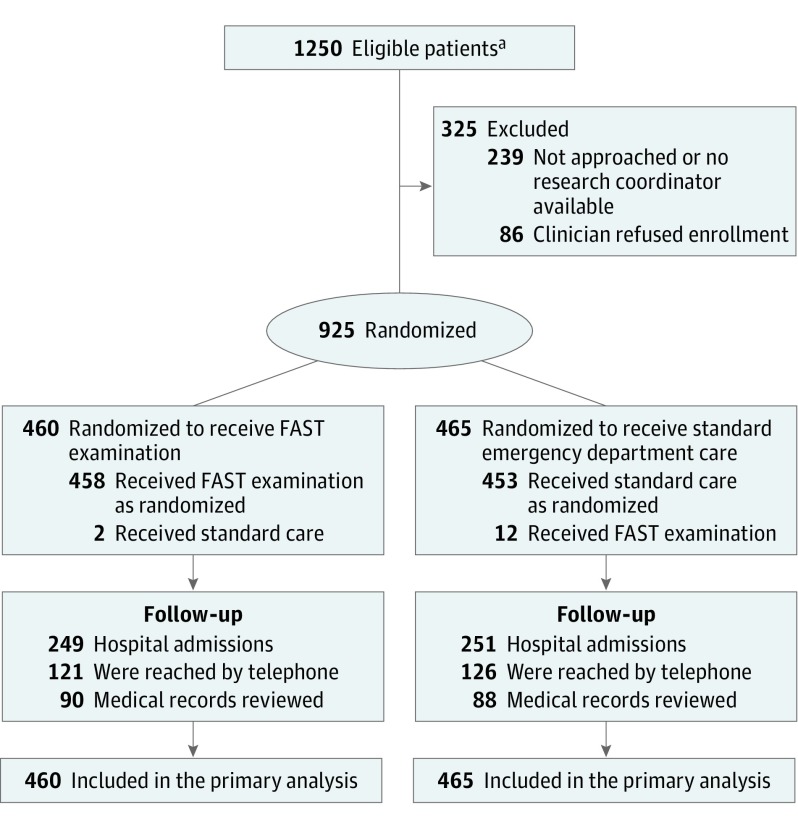
Design, setting, and participants: A randomized clinical trial (April 2012-May 2015) that involved 975 hemodynamically stable children and adolescents younger than 18 years treated for blunt torso trauma at the University of California, Davis Medical Center, a level I trauma center.
Interventions: Patients were randomly assigned to a standard trauma evaluation with the FAST examination by the treating ED physician or a standard trauma evaluation alone.
Main outcomes and measures: Coprimary outcomes were rate of abdominal computed tomographic (CT) scans in the ED, missed intra-abdominal injuries, ED length of stay, and hospital charges.
Results: Among the 925 patients who were randomized (mean [SD] age, 9.7 [5.3] years; 575 males [62%]), all completed the study. A total of 50 patients (5.4%, 95% CI, 4.0% to 7.1%) were diagnosed with intra-abdominal injuries, including 40 (80%; 95% CI, 66% to 90%) who had intraperitoneal fluid found on an abdominal CT scan, and 9 patients (0.97%; 95% CI, 0.44% to 1.8%) underwent laparotomy. The proportion of patients with abdominal CT scans was 241 of 460 (52.4%) in the FAST group and 254 of 465 (54.6%) in the standard care-only group (difference, -2.2%; 95% CI, -8.7% to 4.2%). One case of missed intra-abdominal injury occurred in a patient in the FAST group and none in the control group (difference, 0.2%; 95% CI, -0.6% to 1.2%). The mean ED length of stay was 6.03 hours in the FAST group and 6.07 hours in the standard care-only group (difference, -0.04 hours; 95% CI, -0.47 to 0.40 hours). Median hospital charges were $46 415 in the FAST group and $47 759 in the standard care-only group (difference, -$1180; 95% CI, -$6651 to $4291).
Conclusions and relevance: Among hemodynamically stable children treated in an ED following blunt torso trauma, the use of FAST compared with standard care only did not improve clinical care, including use of resources; ED length of stay; missed intra-abdominal injuries; or hospital charges. These findings do not support the routine use of FAST in this setting.
Trial registration: clinicaltrials.gov Identifier: NCT01540318.
Conflict of interest statement
Figures
Comment in
-
Abdominal Ultrasound for Pediatric Blunt Trauma: FAST Is Not Always Better.JAMA. 2017 Jun 13;317(22):2283-2285. doi: 10.1001/jama.2017.6163. JAMA. 2017. PMID: 28609517 No abstract available.
-
The FAST Examination for Children With Abdominal Trauma.JAMA. 2017 Oct 10;318(14):1394. doi: 10.1001/jama.2017.12943. JAMA. 2017. PMID: 29049578 No abstract available.
-
Not so FAST-let's not abandon the pediatric focused assessment with sonography in trauma yet.J Thorac Dis. 2018 Jan;10(1):1-3. doi: 10.21037/jtd.2017.12.37. J Thorac Dis. 2018. PMID: 29600007 Free PMC article. No abstract available.
References
-
- Ma OJ, Mateer JR, Ogata M, Kefer MP, Wittmann D, Aprahamian C. Prospective analysis of a rapid trauma ultrasound examination performed by emergency physicians. J Trauma. 1995;38(6):879-885. - PubMed
-
- Rozycki GS, Ochsner MG, Jaffin JH, Champion HR. Prospective evaluation of surgeons’ use of ultrasound in the evaluation of trauma patients. J Trauma. 1993;34(4):516-526. - PubMed
-
- Holmes JF, Gladman A, Chang CH. Performance of abdominal ultrasonography in pediatric blunt trauma patients: a meta-analysis. J Pediatr Surg. 2007;42(9):1588-1594. - PubMed
-
- Melniker LA, Leibner E, McKenney MG, Lopez P, Briggs WM, Mancuso CA. Randomized controlled clinical trial of point-of-care, limited ultrasonography for trauma in the emergency department. Ann Emerg Med. 2006;48(3):227-235. - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
