

Pembrolizumab-Induced Thyroiditis: Comprehensive Clinical Review and Insights Into Underlying Involved Mechanisms
- PMID: 28609832
- PMCID: PMC5546861
- DOI: 10.1210/jc.2017-00448
Pembrolizumab-Induced Thyroiditis: Comprehensive Clinical Review and Insights Into Underlying Involved Mechanisms
Abstract
Context: Thyroid immune-related adverse events (irAEs) in patients treated with programmed death receptor-1 (PD-1) blockade are increasingly recognized as one of the most common adverse effects. Our aim was to determine the incidence and examine the potential mechanisms of anti-PD-1-induced thyroid irAEs.
Design: Single-center, retrospective cohort study.
Patients and measurements: We studied 93 patients with advanced cancer (ages 24 to 82 years; 60% males) who received at least one infusion of pembrolizumab. Thyroid test results and thyroid imaging modalities were reviewed. Comprehensive 10-color flow cytometry of peripheral blood was performed.
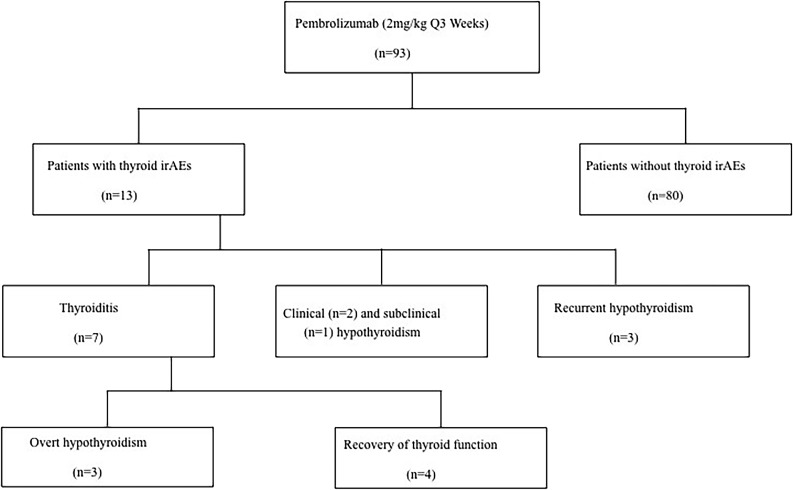
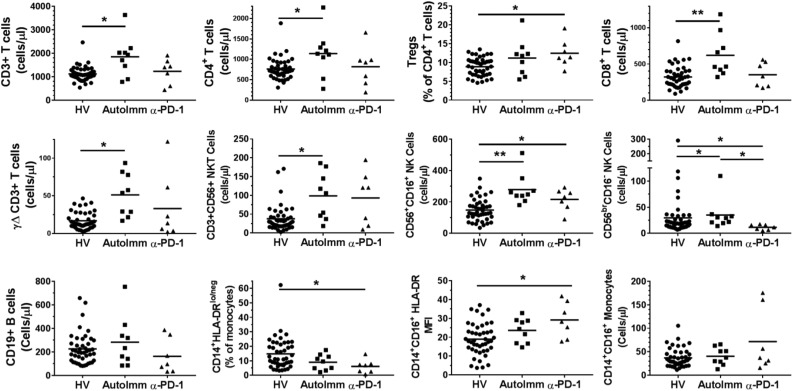
Results: Thirteen (14%) thyroid irAEs were observed. Thyroiditis occurred in seven patients (54%), from which four recovered. New onset of hypothyroidism overt/subclinical developed in three patients. Levothyroxine dosing required doubling in three patients with a known history of hypothyroidism. Thyroperoxidase antibodies were positive in the minority of the patients [4/13 (31%)] and diffuse increased 18fludeoxyglucose uptake of the thyroid gland was observed in the majority [7/11 (64%)] of patients. We observed more circulating CD56+CD16+ natural killer (NK) cells and an elevated HLA-DR surface expression in the inflammatory intermediate CD14+CD16+ monocytes in anti-PD-1-treated patients.
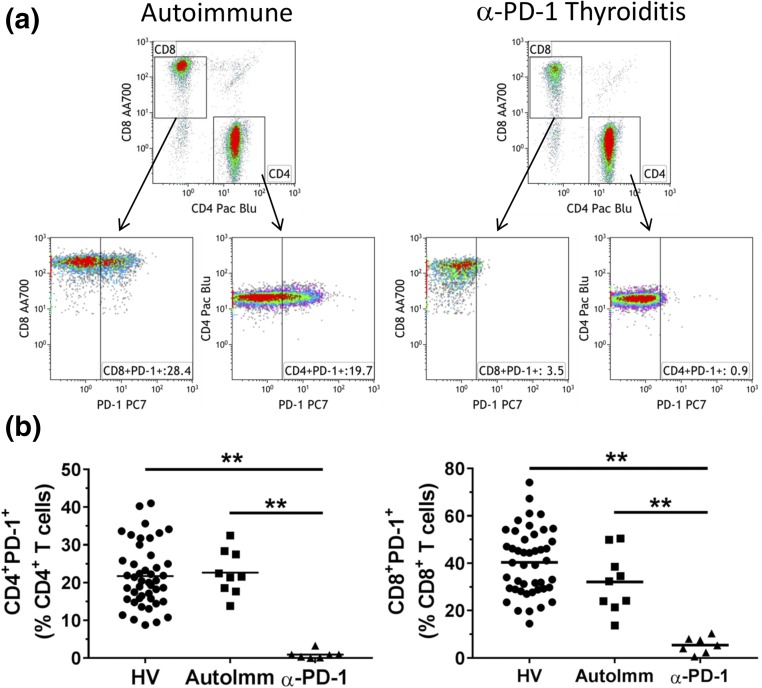
Conclusions: Thyroid dysfunction is common in cancer patients treated with pembrolizumab. Reversible destructive thyroiditis and overt hypothyroidism are the most common clinical presentations. The mechanism of thyroid destruction appears independent of thyroid autoantibodies and may include T cell, NK cell, and/or monocyte-mediated pathways. Because the thyroid is a frequent target of anti-PD-1 therapies, patients with therapeutically refractory thyroid cancer may be ideal candidates for this treatment.
Copyright © 2017 Endocrine Society
Figures
References
-
- Hodi FS, O’Day SJ, McDermott DF, Weber RW, Sosman JA, Haanen JB, Gonzalez R, Robert C, Schadendorf D, Hassel JC, Akerley W, van den Eertwegh AJ, Lutzky J, Lorigan P, Vaubel JM, Linette GP, Hogg D, Ottensmeier CH, Lebbé C, Peschel C, Quirt I, Clark JI, Wolchok JD, Weber JS, Tian J, Yellin MJ, Nichol GM, Hoos A, Urba WJ. Improved survival with ipilimumab in patients with metastatic melanoma. N Engl J Med. 2010;363(8):711–723. - PMC - PubMed
-
- Schadendorf DHF, Hodi FS, Robert C, Weber JS, Margolin K, Hamid O, Patt D, Chen T-T, Berman DM, Wolchok JD. Pooled analysis of long-term survival data from phase II and phase III trials of ipilimumab in metastatic or locally advanced unresectable melanoma. J Clin Oncol. 2015;33(17):1889–1894. - PMC - PubMed
-
- Robert C, Ribas A, Wolchok JD, Hodi FS, Hamid O, Kefford R, Weber JS, Joshua AM, Hwu WJ, Gangadhar TC, Patnaik A, Dronca R, Zarour H, Joseph RW, Boasberg P, Chmielowski B, Mateus C, Postow MA, Gergich K, Elassaiss-Schaap J, Li XN, Iannone R, Ebbinghaus SW, Kang SP, Daud A. Anti-programmed-death-receptor-1 treatment with pembrolizumab in ipilimumab-refractory advanced melanoma: a randomised dose-comparison cohort of a phase 1 trial. Lancet. 2014;384(9948):1109–1117. - PubMed
-
- Robert C, Schachter J, Long GV, Arance A, Grob JJ, Mortier L, Daud A, Carlino MS, McNeil C, Lotem M, Larkin J, Lorigan P, Neyns B, Blank CU, Hamid O, Mateus C, Shapira-Frommer R, Kosh M, Zhou H, Ibrahim N, Ebbinghaus S, Ribas A; KEYNOTE-006 investigators . Pembrolizumab versus ipilimumab in advanced melanoma. N Engl J Med. 2015;372(26):2521–2532. - PubMed
-
- Wolchok JD, Kluger H, Callahan MK, Postow MA, Rizvi NA, Lesokhin AM, Segal NH, Ariyan CE, Gordon RA, Reed K, Burke MM, Caldwell A, Kronenberg SA, Agunwamba BU, Zhang X, Lowy I, Inzunza HD, Feely W, Horak CE, Hong Q, Korman AJ, Wigginton JM, Gupta A, Sznol M. Nivolumab plus ipilimumab in advanced melanoma. N Engl J Med. 2013;369(2):122–133. - PMC - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
