

The Diagnosis and Treatment of Sjögren's Syndrome
- PMID: 28610655
- PMCID: PMC5471601
- DOI: 10.3238/arztebl.2017.0354
The Diagnosis and Treatment of Sjögren's Syndrome
Abstract
Background: Sjögren's syndrome is one of the more common inflammatory rheumatological diseases, with a prevalence of at least 0.4% in Germany.
Methods: This review is based on pertinent articles retrieved by a selective search in PubMed. Special attention is drawn to updated classification criteria and current treatment recommendations.
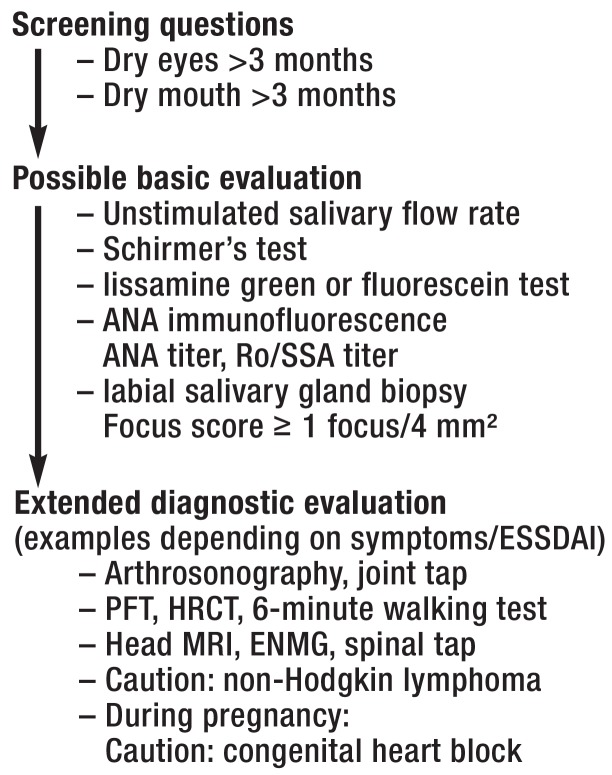
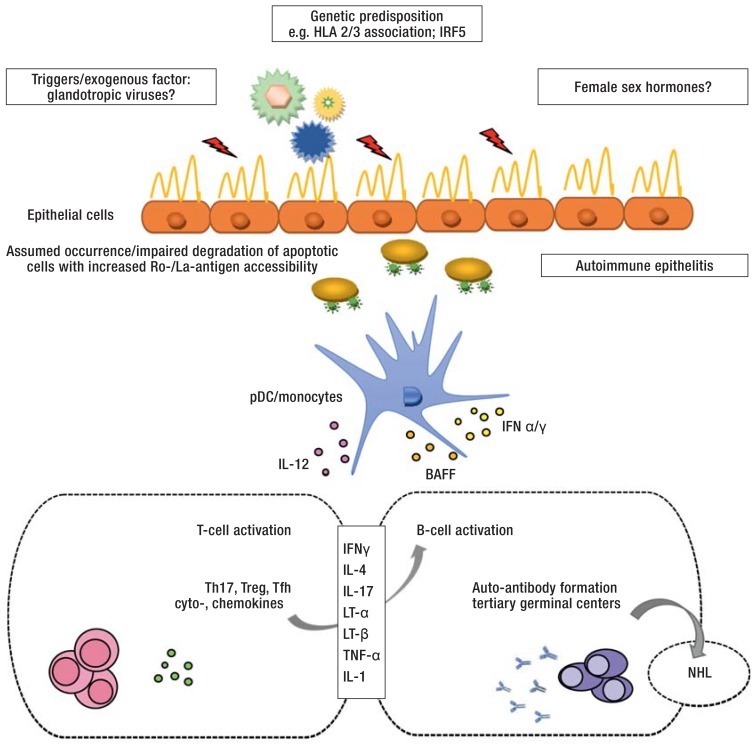
Results: Sjögren's syndrome has a wide variety of presentations, ranging from the local involvement of exocrine glands with keratoconjunctivitis sicca and xerostomia (the leading signs of the disease) to the systemic, extraglandular involvement of multiple organs. Fatigue also markedly worsens the patients' quality of life. Serologic testing reveals antinuclear auto-antibodies (anti-Ro/ SSA and anti-La/SSB) as well as rheumatoid factors. The histological hallmark of the disease is focal lymphocytic infiltration in otherwise normal-appearing glandular acini. The disease also markedly elevates the risk of non-Hodgkin lymphoma of the B-cell series, which arises in about 5% of patients. Primary Sjögren's syndrome (pSS) differs from the secondary form (sSS), which appears in the setting of another autoimmune disease, particularly systemic lupus erythematosus (15-36%), rheumatoid arthritis (20-32%), and limited or progressive systemic sclerosis (11-24%). Disease-modifying therapy is reserved for patients with systemic involvement; there is limited evidence for its efficacy. Because of the complexity of this disease, some of its clinical manifestations may require interdisciplinary treatment.
Conclusion: The main considerations in the interdisciplinary care of patients with Sjögren's disease are measures to improve quality of life, pharmacological and non-pharmacological treatments to keep disease activity in check, and management of the risk of lymphoma. Future therapeutic approaches must take the heterogeneity of the disease into account.
Figures
Comment in
-
Filamentary Keratitis as Indication.Dtsch Arztebl Int. 2017 Sep 29;114(39):660. doi: 10.3238/arztebl.2017.0660a. Dtsch Arztebl Int. 2017. PMID: 29034868 Free PMC article. No abstract available.
-
Further Symptoms of Sjögren's Syndrome.Dtsch Arztebl Int. 2017 Sep 29;114(39):660. doi: 10.3238/arztebl.2017.0660b. Dtsch Arztebl Int. 2017. PMID: 29034869 Free PMC article. No abstract available.
References
-
- Tomiak C, Dorner T. Sjogren’s syndrome. Current aspects from a rheumatological point of view. Z Rheumatol. 2006;65:505–517. - PubMed
-
- Qin B, Wang J, Yang Z, et al. Epidemiology of primary Sjögren’s syndrome: a systematic review and meta-analysis. Ann Rheum Dis. 2015;74:1983–1989. - PubMed
-
- Westhoff G, Zink A. Epidemiology of primary Sjogren’s syndrome. Z Rheumatol. 2010;69:41–49. - PubMed
-
- Brito-Zeron P, Theander E, Baldini C, et al. Early diagnosis of primary Sjögren’s syndrome: EULAR-SS task force clinical recommendations. Expert Rev Clin Immunol. 2016;12:137–156. - PubMed
-
- Fox PC, Bowman SJ, Segal B, et al. Oral involvement in primary Sjögren syndrome. J Am Dent Assoc. 2008;139:1592–1601. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials