

Inhibition of Renal Sodium-Glucose Cotransport With Empagliflozin Lowers Fasting Plasma Glucose and Improves β-Cell Function in Subjects With Impaired Fasting Glucose
- PMID: 28611037
- PMCID: PMC7301341
- DOI: 10.2337/db17-0055
Inhibition of Renal Sodium-Glucose Cotransport With Empagliflozin Lowers Fasting Plasma Glucose and Improves β-Cell Function in Subjects With Impaired Fasting Glucose
Abstract
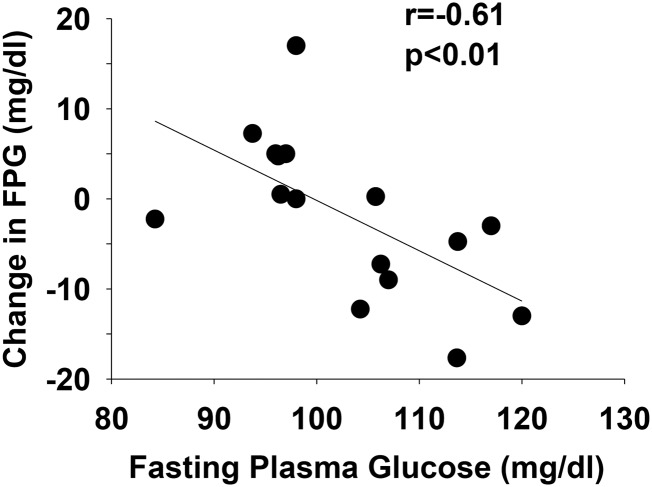
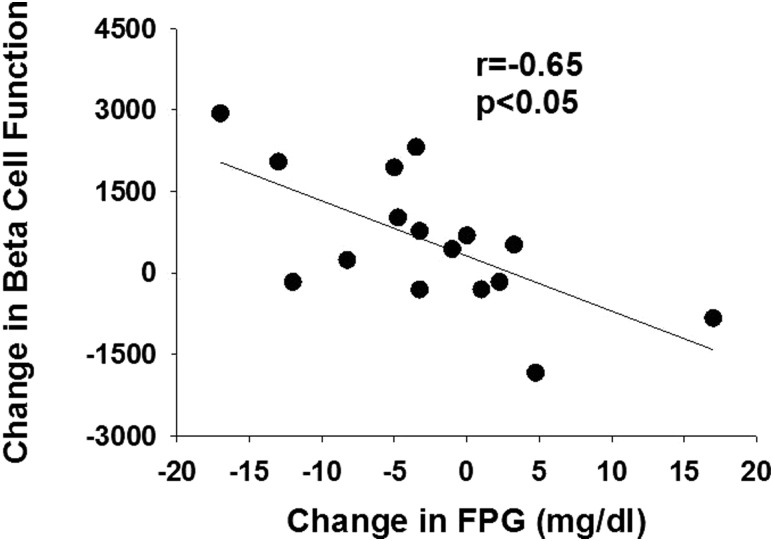
The objective of this study was to examine the effect of renal sodium-glucose cotransporter inhibition with empagliflozin on the fasting plasma glucose (FPG) concentration and β-cell function in subjects with impaired fasting glucose (IFG). Eight subjects with normal fasting glucose (NFG) and eight subjects with IFG received empagliflozin (25 mg/day) for 2 weeks. FPG concentration and β-cell function was measured with a nine-step hyperglycemic clamp before and 48 h and 14 days after the start of empagliflozin. Empagliflozin caused 50 ± 4 and 45 ± 4 g glucosuria on day 2 in subjects with IFG and NFG, respectively, and the glucosuria was maintained for 2 weeks in both groups. The FPG concentration decreased only in subjects with IFG from 110 ± 2 to 103 ± 3 mg/dL (P < 0.01) after 14 days. The FPG concentration remained unchanged (95 ± 2 to 94 ± 2 mg/dL) in subjects with NFG. Empagliflozin enhanced β-cell function only in subjects with IFG. The incremental area under the plasma C-peptide concentration curve during the hyperglycemic clamp increased by 22 ± 4 and 23 ± 4% after 48 h and 14 days, respectively (P < 0.01); the plasma C-peptide response remained unchanged in subjects with NFG. Insulin sensitivity during the hyperglycemic clamp was not affected by empagliflozin in either IFG or NFG. Thus, β-cell function measured with the insulin secretion/insulin sensitivity (disposition) index increased significantly in IFG, but not in subjects with normal glucose tolerance. Inhibition of renal sodium-glucose cotransport with empagliflozin in subjects with IFG and NFG produces comparable glucosuria but lowers the plasma glucose concentration and improves β-cell function only in subjects with IFG.
Trial registration: ClinicalTrials.gov NCT01867307.
© 2017 by the American Diabetes Association.
Figures



References
-
- The Expert Committee on the Diagnosis and Classification of Diabetes Mellitus Report of the Expert Committee on the Diagnosis and Classification of Diabetes Mellitus. Diabetes Care 1997;20:1183–1197 - PubMed
-
- Unwin N, Shaw J, Zimmet P, Alberti KG. Impaired glucose tolerance and impaired fasting glycaemia: the current status on definition and intervention. Diabet Med 2002;19:708–723 - PubMed
-
- Abdul-Ghani MA, Tripathy D, DeFronzo RA. Contributions of beta-cell dysfunction and insulin resistance to the pathogenesis of impaired glucose tolerance and impaired fasting glucose. Diabetes Care 2006;29:1130–1139 - PubMed
-
- Pratley RE, Weyer C. The role of impaired early insulin secretion in the pathogenesis of Type II diabetes mellitus. Diabetologia 2001;44:929–945 - PubMed
-
- Gastaldelli A, Ferrannini E, Miyazaki Y, Matsuda M, DeFronzo RA; San Antonio metabolism study . Beta-cell dysfunction and glucose intolerance: results from the San Antonio metabolism (SAM) study. Diabetologia 2004;47:31–39 - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
