

Association of Polymorphisms in Pharmacogenetic Candidate Genes with Propofol Susceptibility
- PMID: 28611364
- PMCID: PMC5469860
- DOI: 10.1038/s41598-017-03229-3
Association of Polymorphisms in Pharmacogenetic Candidate Genes with Propofol Susceptibility
Abstract
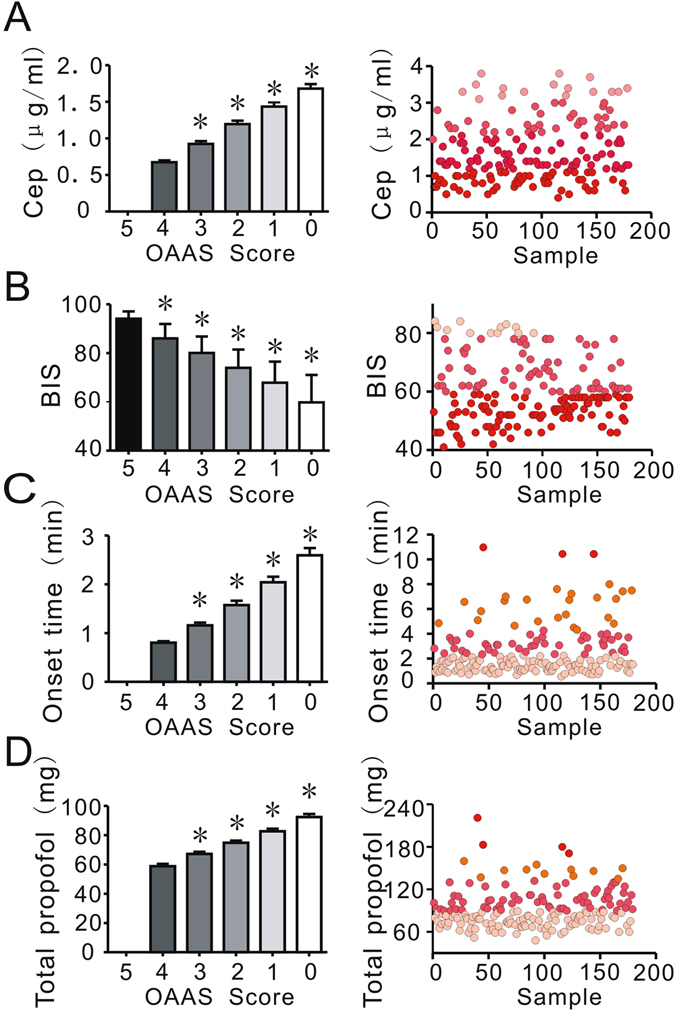
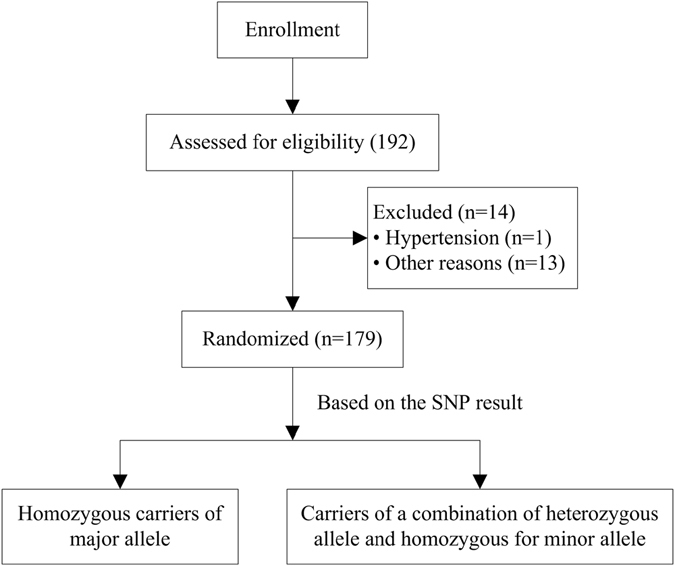
Significant individual susceptibility to intravenous anesthetic propofol exists. The etiology of individual variability in the response to propofol may be influenced by genetic polymorphisms in metabolic and functional pathways. With current pharmacogenetics and modern molecular biology technologies, it is possible to study the influence of genetic polymorphisms on susceptibility to propofol. When inducing general anesthesia with intravenous propofol, high individual susceptibility to propofol was found. Using Sequenom MassARRAY single-nucleotide polymorphism (SNP) genotyping, we identified a mutation (rs6313) in the 5HT2A gene that was correlated to individual susceptibility to propofol effect-site concentration (Cep) and onset time of propofol induction. Carriers of the minor allele (G) of 5HT2A rs6313 required less propofol (20% decrease in Cep) and less time (40% decrease in onset time) to induce anesthesia. Moreover, associations were found between the gamma-aminobutyric acid (GABA) receptor SNP rs2279020 and the SCN9A SNP rs6746030 and the susceptibility of bispectral index (BIS) after propofol-induced anesthesia. In addition, dominant mutations in GABAA1 rs2279020, GABAA2 rs11503014, and CHRM2 rs1824024 were putatively associated with cardiovascular susceptibility to propofol anesthesia. No gene-gene interactions were found through a standardized measure of linkage disequilibrium and a multifactor dimensionality reduction analysis. Our results suggest that genetic polymorphisms related to mechanisms of propofol anesthesia are involved in propofol susceptibility.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

Similar articles
-
An investigation of potential genetic determinants of propofol requirements and recovery from anaesthesia.Eur J Anaesthesiol. 2007 Nov;24(11):912-9. doi: 10.1017/S0265021507000476. Epub 2007 Jun 7. Eur J Anaesthesiol. 2007. PMID: 17555608
-
A conserved tyrosine in the beta2 subunit M4 segment is a determinant of gamma-aminobutyric acid type A receptor sensitivity to propofol.Anesthesiology. 2007 Sep;107(3):412-8. doi: 10.1097/01.anes.0000278875.36639.2c. Anesthesiology. 2007. PMID: 17721243
-
Influence of Potential Gene Polymorphisms on Propofol Dosage Regimen in Patients Undergoing Abdominal Hysterectomy.Balkan J Med Genet. 2021 Mar 23;23(2):41-48. doi: 10.2478/bjmg-2020-0030. eCollection 2020 Nov. Balkan J Med Genet. 2021. PMID: 33816071 Free PMC article.
-
Actions of Propofol on Neurons in the Cerebral Cortex.J Nippon Med Sch. 2017;84(4):165-169. doi: 10.1272/jnms.84.165. J Nippon Med Sch. 2017. PMID: 28978896 Review.
-
Clinical Importance of Potential Genetic Determinants Affecting Propofol Pharmacokinetics and Pharmacodynamics.Front Med (Lausanne). 2022 Feb 28;9:809393. doi: 10.3389/fmed.2022.809393. eCollection 2022. Front Med (Lausanne). 2022. PMID: 35295593 Free PMC article. Review.
Cited by
-
Genetic polymorphisms are associated with individual susceptibility to dexmedetomidine.Front Genet. 2023 Aug 24;14:1187415. doi: 10.3389/fgene.2023.1187415. eCollection 2023. Front Genet. 2023. PMID: 37693312 Free PMC article.
-
The Effects of Gene Variations of GABRA2, GABRB1, GABRG2, GAD1 and SLC1A3 on Patients with Propofol During Anesthesia Induction.Pharmgenomics Pers Med. 2021 Sep 17;14:1185-1192. doi: 10.2147/PGPM.S326885. eCollection 2021. Pharmgenomics Pers Med. 2021. PMID: 34557020 Free PMC article.
-
Are Genome-wide Association Studies Worth the Trouble?Anesthesiology. 2024 Aug 1;141(2):214-216. doi: 10.1097/ALN.0000000000005074. Anesthesiology. 2024. PMID: 38980159 Free PMC article. No abstract available.
-
Impact of propofol on gastrointestinal cancer outcomes: A review of cellular behavior, growth, and metastasis.World J Clin Oncol. 2025 Jul 24;16(7):104727. doi: 10.5306/wjco.v16.i7.104727. World J Clin Oncol. 2025. PMID: 40741181 Free PMC article. Review.
-
Polymorphisms of pharmacogenetic candidate genes affect etomidate anesthesia susceptibility.Front Genet. 2022 Sep 28;13:999132. doi: 10.3389/fgene.2022.999132. eCollection 2022. Front Genet. 2022. PMID: 36246646 Free PMC article.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
