

Different techniques for harvesting grafts for living donor liver transplantation: A systematic review and meta-analysis
- PMID: 28611526
- PMCID: PMC5449430
- DOI: 10.3748/wjg.v23.i20.3730
Different techniques for harvesting grafts for living donor liver transplantation: A systematic review and meta-analysis
Abstract
Aim: To perform a systematic review and meta-analysis on minimally vs conventional invasive techniques for harvesting grafts for living donor liver transplantation.
Methods: PubMed, Web of Science, EMBASE, and the Cochrane Library were searched comprehensively for studies comparing MILDH with conventional living donor hepatectomy (CLDH). Intraoperative and postoperative outcomes (operative time, estimated blood loss, postoperative liver function, length of hospital stay, analgesia use, complications, and survival rate) were analyzed in donors and recipients. Articles were included if they: (1) compared the outcomes of MILDH and CLDH; and (2) reported at least some of the above outcomes.
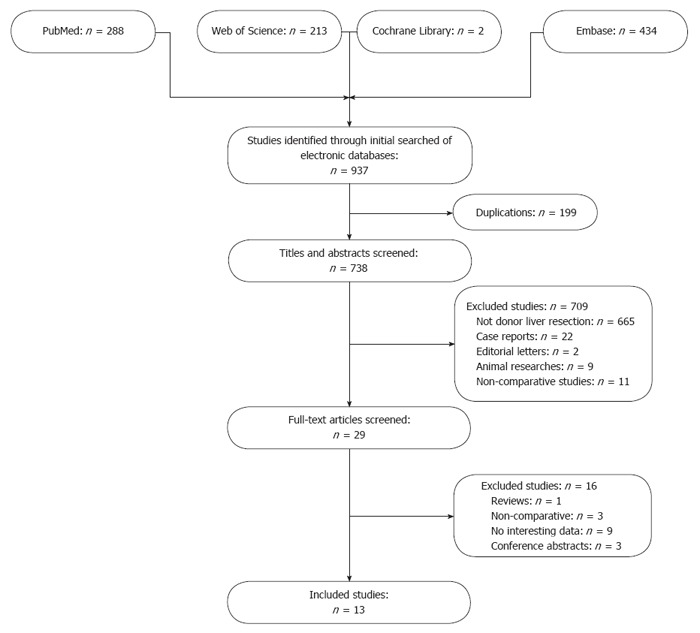
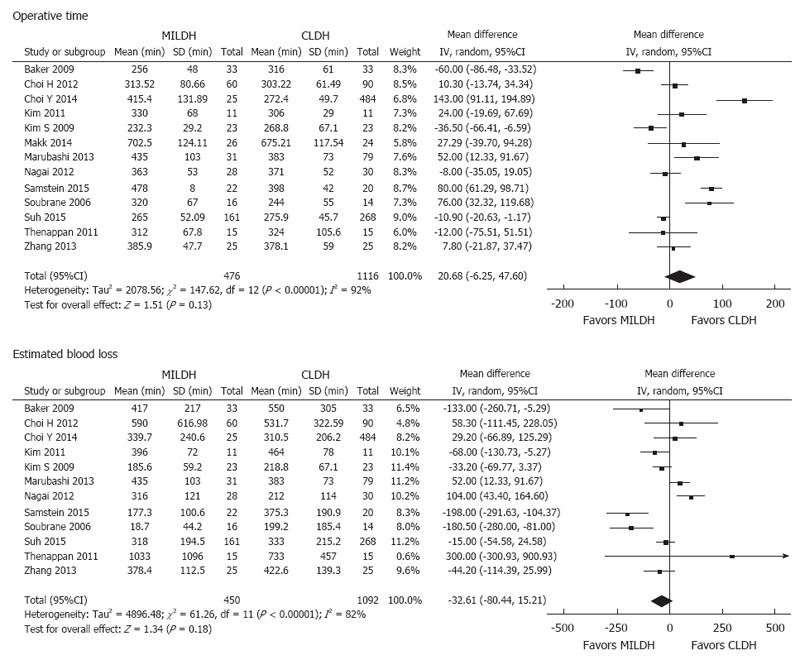
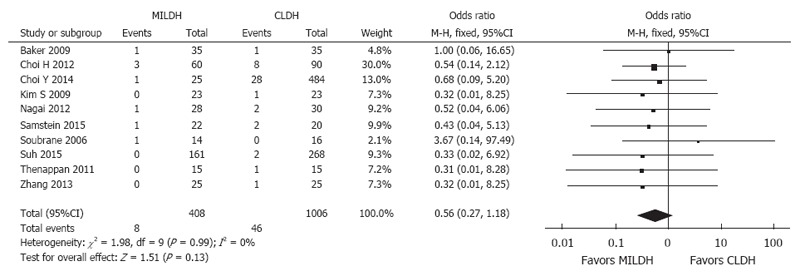
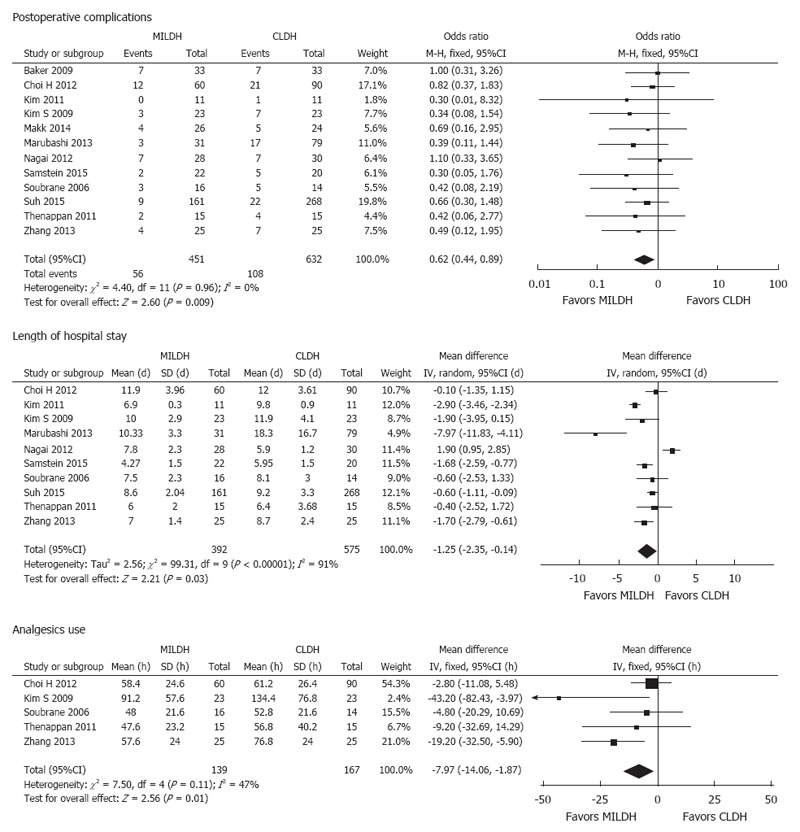
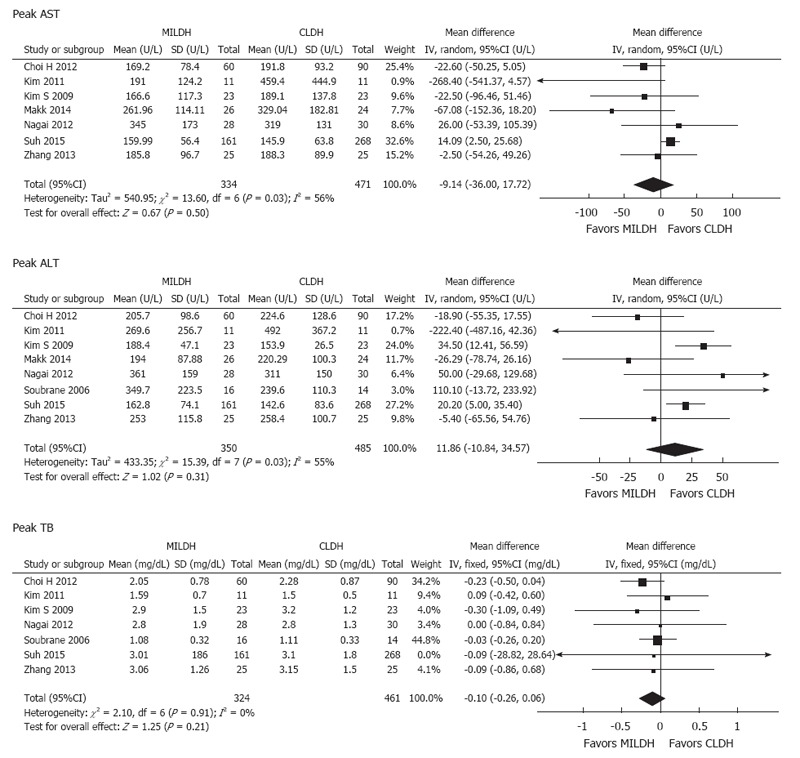
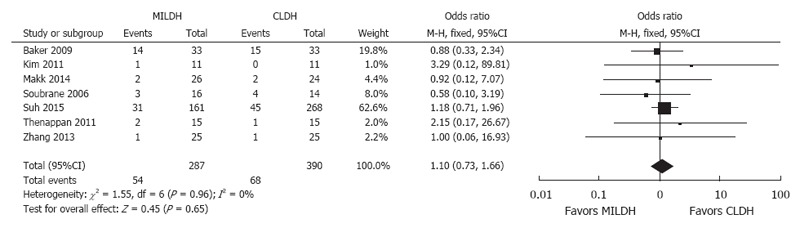
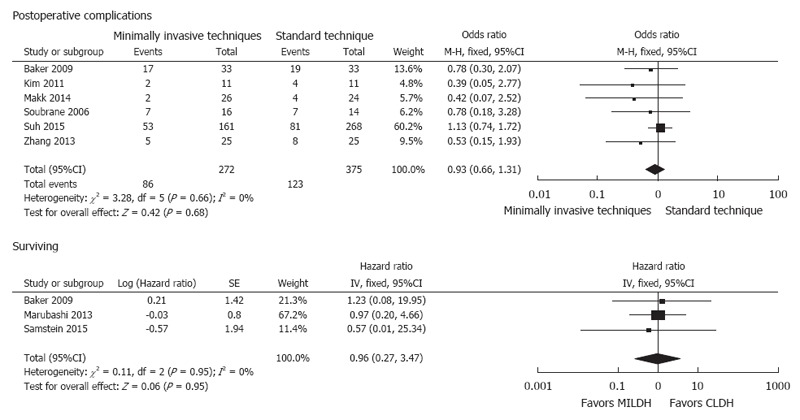
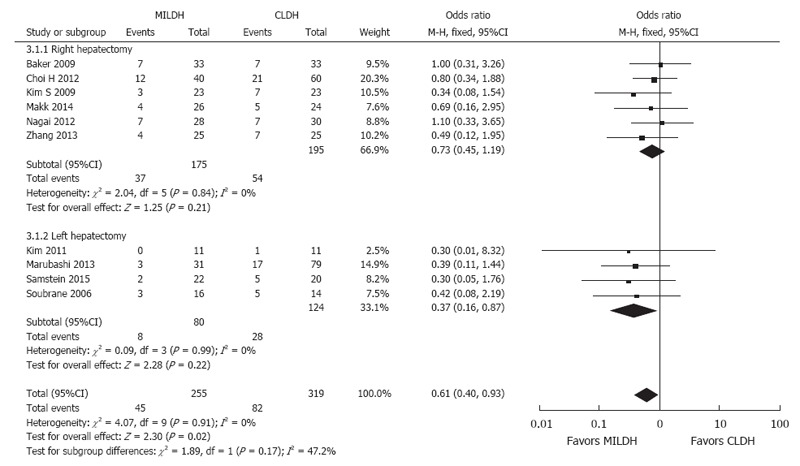
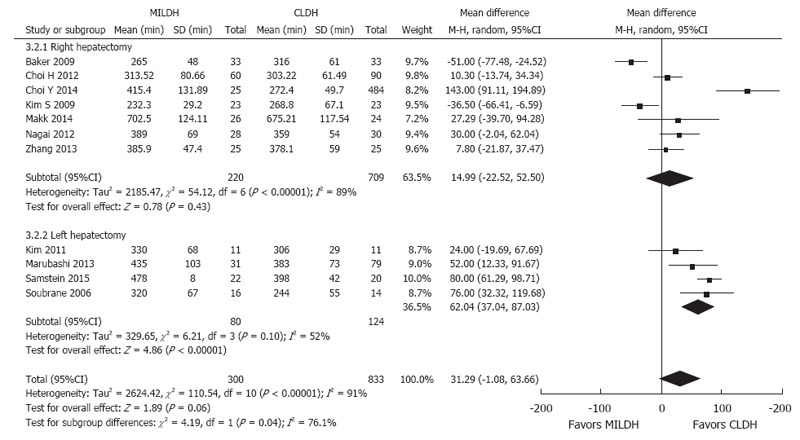
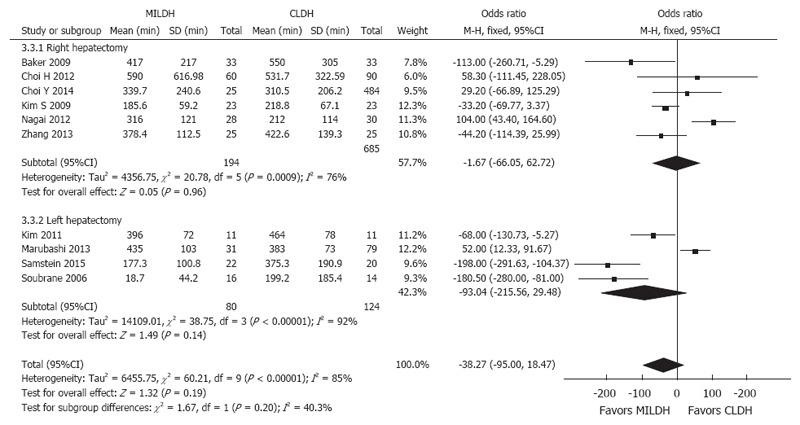
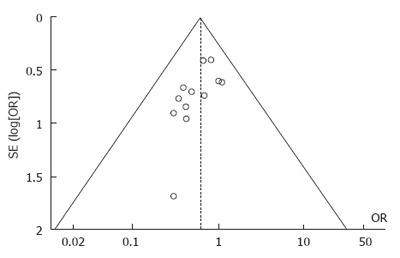
Results: Of 937 articles identified, 13, containing 1592 patients, met our inclusion criteria and were included in the meta-analysis. For donors, operative time [weighted mean difference (WMD) = 20.68, 95%CI: -6.25-47.60, P = 0.13] and blood loss (WMD = -32.61, 95%CI: -80.44-5.21, P = 0.18) were comparable in the two groups. In contrast, analgesia use (WMD = -7.79, 95%CI: -14.06-1.87, P = 0.01), postoperative complications [odds ratio (OR) = 0.62, 95%CI: 0.44-0.89, P = 0.009], and length of hospital stay (WMD): -1.25, 95%CI: -2.35-0.14, P = 0.03) significantly favored MILDH. No differences were observed in recipient outcomes, including postoperative complications (OR = 0.93, 95%CI: 0.66-1.31, P = 0.68) and survival rate (HR = 0.96, 95%CI: 0.27-3.47, P = 0.95). Funnel plot and statistical methods showed a low probability of publication bias.
Conclusion: MILDH is safe, effective, and feasible for living donor liver resection with fewer donor postoperative complications, reduced length of hospital stay and analgesia requirement than CLDH.
Keywords: Conventional invasive approaches; Graft harvesting; Living donor hepatectomy; Meta-analysis; Minimally invasive techniques.
Conflict of interest statement
Conflict-of-interest statement: The authors declare that there is no conflict of interest related to this report.
Figures
References
-
- Strong RW, Lynch SV, Ong TH, Matsunami H, Koido Y, Balderson GA. Successful liver transplantation from a living donor to her son. N Engl J Med. 1990;322:1505–1507. - PubMed
-
- Park JI, Kim KH, Lee SG. Laparoscopic living donor hepatectomy: a review of current status. J Hepatobiliary Pancreat Sci. 2015;22:779–788. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
