

Intra- and Postoperative Electrocochleography May Be Predictive of Final Electrode Position and Postoperative Hearing Preservation
- PMID: 28611574
- PMCID: PMC5447029
- DOI: 10.3389/fnins.2017.00291
Intra- and Postoperative Electrocochleography May Be Predictive of Final Electrode Position and Postoperative Hearing Preservation
Abstract
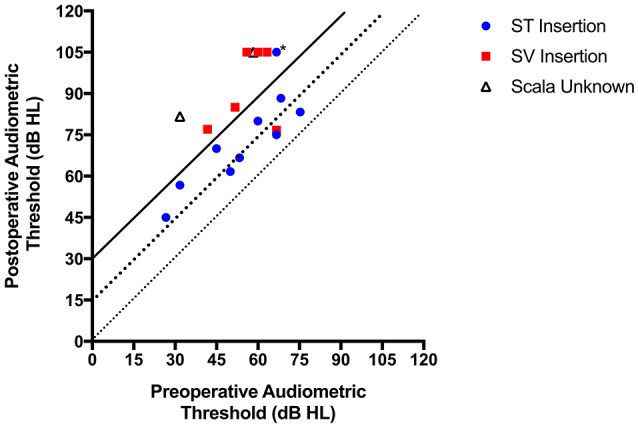
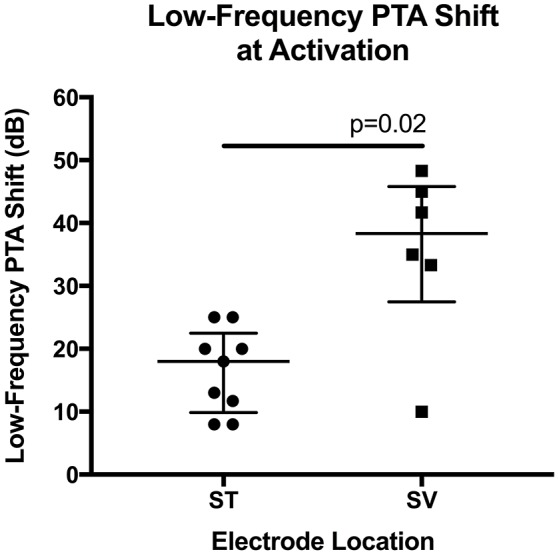
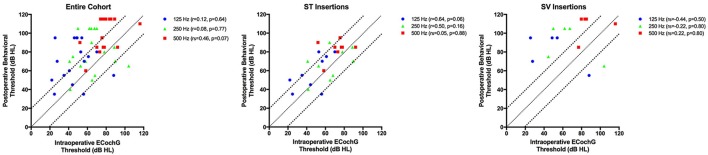
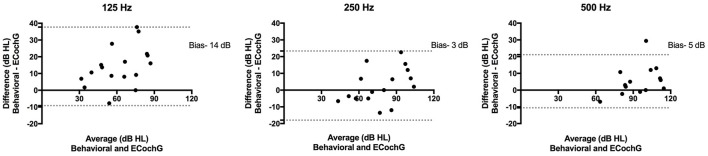
Introduction: The objectives of the current study were to (1) determine the relationship between electrocochleography (ECochG), measured from the cochlear implant (CI) electrode array during and after implantation, and postoperative audiometric thresholds, (2) determine the relationship between ECochG amplitude and electrode scalar location determined by computerized tomography (CT); and (3) determine whether changes in cochlear microphonic (CM) amplitude during electrode insertion were associated with postoperative hearing. Materials and Methods: Eighteen subjects undergoing CI with an Advanced Bionics Mid-Scala device were prospectively studied. ECochG responses were recorded using the implant coupled to a custom signal recording unit. ECochG amplitude collected intraoperatively concurrent with CI insertion and at activation was compared with audiometric thresholds postoperatively. Sixteen patients also underwent postoperative CT to determine scalar location and the relationship to ECochG measures and residual hearing. Results: Mean low-frequency pure tone average (LFPTA) increased following surgery by an average of 28 dB (range 8-50). Threshold elevation was significantly greater for electrodes with scalar dislocation. No correlation was found between intraoperative ECochG and postoperative behavioral thresholds collapsed across frequency; however, mean differences in thresholds measured by intraoperative ECochG and postoperative audiometry were significantly smaller for electrodes inserted completely within scala tympani (ST) vs. those translocating from ST to scala vestibuli. A significant correlation was observed between postoperative ECochG thresholds and behavioral thresholds obtained at activation. Discussion: Postoperative audiometry currently serves as a marker for intracochlear trauma though thresholds are not obtained until device activation or later. When measured at the same time-point postoperatively, low-frequency ECochG thresholds correlated with behavioral thresholds. Intraoperative ECochG thresholds, however, did not correlate significantly with postoperative behavioral thresholds suggesting that changes in cochlear physiology occur between electrode insertion and activation. ECochG may hold clinical utility providing surgeons with feedback regarding insertion trauma due to scalar translocation, which may be predictive of postoperative hearing preservation. Conclusion: CI insertion trauma is generally not evident until postoperative audiometry when loss of residual hearing is confirmed. ECochG has potential to provide estimates of trauma during insertion as well as reliable information regarding degree of hearing preservation.
Keywords: audiometry; cochlear implant; cochlear microphonic; electrocochleography; hearing loss; hearing preservation; residual hearing.
Figures


Similar articles
-
Monitoring Cochlear Health With Intracochlear Electrocochleography During Cochlear Implantation: Findings From an International Clinical Investigation.Ear Hear. 2023 Mar-Apr 01;44(2):358-370. doi: 10.1097/AUD.0000000000001288. Epub 2022 Nov 8. Ear Hear. 2023. PMID: 36395515 Free PMC article.
-
Intra-Cochlear Electrocochleography During Cochear Implant Electrode Insertion Is Predictive of Final Scalar Location.Otol Neurotol. 2018 Sep;39(8):e654-e659. doi: 10.1097/MAO.0000000000001906. Otol Neurotol. 2018. PMID: 30113557 Free PMC article.
-
Intraoperative Intracochlear Electrocochleography and Residual Hearing Preservation Outcomes When Using Two Types of Slim Electrode Arrays in Cochlear Implantation.Otol Neurotol. 2019 Jun;40(5S Suppl 1):S29-S37. doi: 10.1097/MAO.0000000000002212. Otol Neurotol. 2019. PMID: 31225820 Clinical Trial.
-
Correlation Between Electrocochleographic Changes During Surgery and Hearing Outcome in Cochlear Implant Recipients: A Case Report and Systematic Review of the Literature.Otol Neurotol. 2020 Mar;41(3):318-326. doi: 10.1097/MAO.0000000000002506. Otol Neurotol. 2020. PMID: 31834213
-
Bridging the gap: A systematic review of intraoperative electrocochleography during cochlear implantation and preservation of residual hearing.PLoS One. 2025 May 13;20(5):e0323493. doi: 10.1371/journal.pone.0323493. eCollection 2025. PLoS One. 2025. PMID: 40359384 Free PMC article.
Cited by
-
Patterns Seen During Electrode Insertion Using Intracochlear Electrocochleography Obtained Directly Through a Cochlear Implant.Otol Neurotol. 2017 Dec;38(10):1415-1420. doi: 10.1097/MAO.0000000000001559. Otol Neurotol. 2017. PMID: 28953607 Free PMC article.
-
Electrocochleography in cochlear implantation: Development, applications, and future directions.World J Otorhinolaryngol Head Neck Surg. 2020 Jun 4;7(2):94-100. doi: 10.1016/j.wjorl.2020.04.006. eCollection 2021 Apr. World J Otorhinolaryngol Head Neck Surg. 2020. PMID: 33997718 Free PMC article. Review. No abstract available.
-
Two different methods to digitally visualize continuous electrocochleography potentials during cochlear implantation: a first description of feasibility.Eur Arch Otorhinolaryngol. 2024 Jun;281(6):2913-2920. doi: 10.1007/s00405-023-08400-3. Epub 2024 Jan 3. Eur Arch Otorhinolaryngol. 2024. PMID: 38170210 Free PMC article.
-
Electrocochleography and cognition are important predictors of speech perception outcomes in noise for cochlear implant recipients.Sci Rep. 2022 Feb 23;12(1):3083. doi: 10.1038/s41598-022-07175-7. Sci Rep. 2022. PMID: 35197556 Free PMC article.
-
Multi-Frequency Electrocochleography and Electrode Scan to Identify Electrode Insertion Trauma during Cochlear Implantation.Brain Sci. 2023 Feb 15;13(2):330. doi: 10.3390/brainsci13020330. Brain Sci. 2023. PMID: 36831873 Free PMC article.
References
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous