

The Economics of an Admissions Holding Unit
- PMID: 28611873
- PMCID: PMC5468058
- DOI: 10.5811/westjem.2017.4.32740
The Economics of an Admissions Holding Unit
Abstract
Introduction: With increasing attention to the actual cost of delivering care, return-on-investment calculations take on new significance. Boarded patients in the emergency department (ED) are harmful to clinical care and have significant financial opportunity costs. We hypothesize that investment in an admissions holding unit for admitted ED patients not only captures opportunity cost but also significantly lowers direct cost of care.
Methods: This was a three-phase study at a busy urban teaching center with significant walkout rate. We first determined the true cost of maintaining a staffed ED bed for one patient-hour and compared it to alternative settings. The opportunity cost for patients leaving without being seen was then conservatively estimated. Lastly, a convenience sample of admitted patients boarding in the ED was observed continuously from one hour after decision-to-admit until physical departure from the ED to capture a record of every interaction with a nurse or physician.
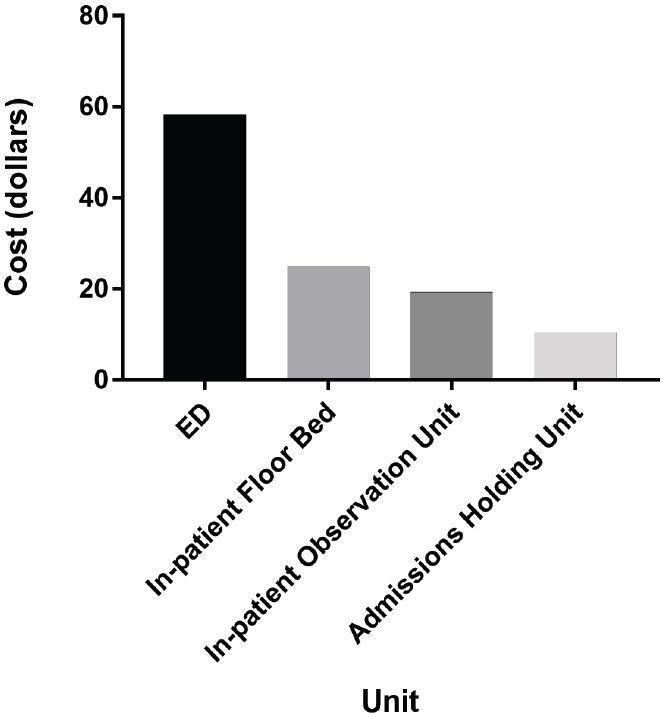
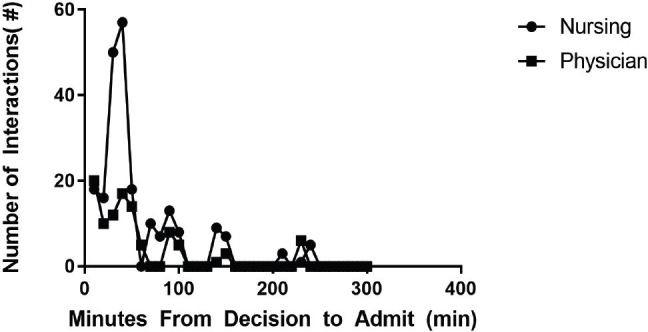
Results: Personnel costs per patient bed-hour were $58.20 for the ED, $24.80 for an inpatient floor, $19.20 for the inpatient observation unit, and $10.40 for an admissions holding area. An eight-bed holding unit operating at practical capacity would free 57.4 hours of bed space in the ED and allow treatment of 20 additional patients. This could yield increased revenues of $27,796 per day and capture opportunity cost of $6.09 million over 219 days, in return for extra staffing costs of $218,650. Analysis of resources used for boarded patients was determined by continuous observation of a convenience sample of ED-boarded patients, which found near-zero interactions with both nursing and physicians during the boarding interval.
Conclusion: Resource expense per ED bed-hour is more than twice that in non-critical care inpatient units. Despite the high cost of available resources, boarded non-critical patients receive virtually no nursing or physician attention. An admissions holding unit is remarkably effective in avoiding the mismatch of the low-needs patients in high-cost care venues. Return on investment is enormous, but this assumes existing clinical space for this unit.
Conflict of interest statement
Conflicts of Interest: By the WestJEM article submission agreement, all authors are required to disclose all affiliations, funding sources and financial or management relationships that could be perceived as potential sources of bias. No author has professional or financial relationships with any companies that are relevant to this study. There are no conflicts of interest or sources of funding to declare.
Figures
References
-
- Kellermann AL. Crisis in the emergency department. N Engl J Med. 2006;355(13):1300–3. - PubMed
-
- Handel DA, Hilton JA, Ward MJ, et al. Emergency department throughput, crowding, and financial outcomes for hospitals. Acad Emerg Med. 2010;17(8):840–7. - PubMed
-
- Moskop JC, Sklar DP, Geiderman JM, et al. Emergency department crowding, part 1--concept, causes, and moral consequences. Ann Emerg Med. 2009;53(5):605–11. - PubMed
-
- Bernstein SL, Aronsky D, Duseja R, et al. The effect of emergency department crowding on clinically oriented outcomes. Acad Emerg Med. 2009;16(1):1–10. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources