

Management of Orbital and Periorbital Venous Malformation
- PMID: 28611988
- PMCID: PMC5447072
- DOI: 10.3389/fsurg.2017.00027
Management of Orbital and Periorbital Venous Malformation
Abstract
Background: To review our management of common venous malformation (VM) affecting the orbit and/or periorbital area.
Methods: Consecutive patients with orbital and/or periorbital VM were identified from our vascular anomalies database. Demographic details of the patients, anatomic site(s) affected, symptoms and signs, presence of a family history of VM, and types of treatment(s) were collected, supplemented by chart review.
Results: A total of 24 patients' age 1-68 (mean, 30) years with orbital and/or periorbital VM presented with cosmetic concerns (n = 17, 71%), distensibility (n = 15, 63%), pain (n = 9, 38%), diplopia (n = 4, 17%), and spontaneous thrombosis (n = 1, 8%). The VM caused globe dystopia (n = 13, 54%), enophthalmos (n = 6, 25%), proptosis (n = 3, 12%), exotropia (n = 3, 12%), and pseudoptosis with visual obstruction (n = 3, 13%). A total of 11 (46%) patients were managed conservatively. 13 (54%) patients underwent active treatment. Ethanol sclerotherapy (ES) was performed in six patients with extensive facial VM associated with orbital/periorbital involvement, resulting in symptomatic improvement in five patients, one of whom developed skin necrosis and another patient developed reduced infraorbital nerve sensation. Surgery was performed for localized lesion (n = 3, 23%), for extensive lesions (n = 4, 31%) and as an adjunct to ES (n = 6, 46%) resulting in symptomatic improvement in all patients. One patient required correction of lower lid ectropion.
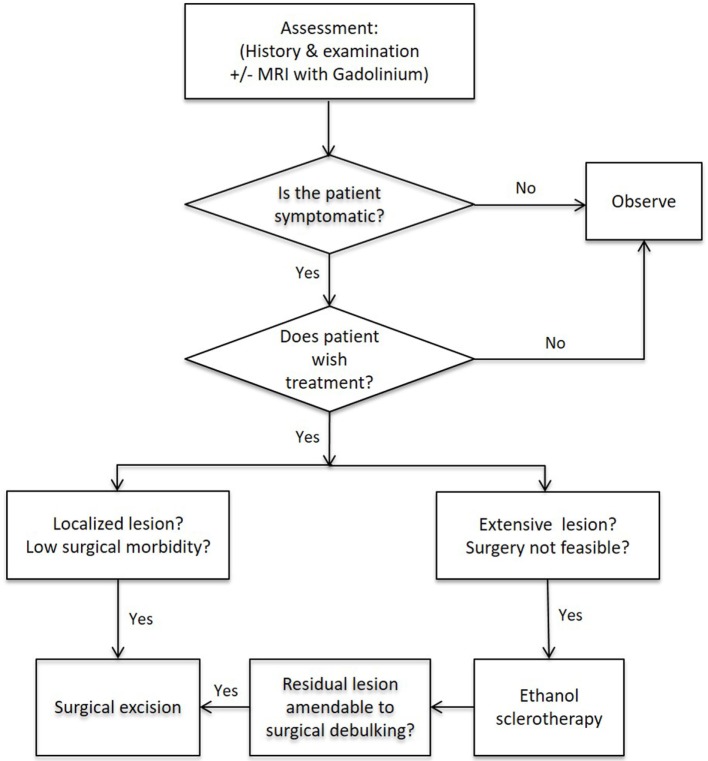
Conclusion: Orbital and/or periorbital VMs are heterogeneous, and management needs to be individualized. Surgery is used for localized lesions aiming for complete excision, as a debulking procedure for extensive orbital/periorbital VM when ES was not possible, or following ES for extensive facial VM with orbital and/or periorbital involvement.
Keywords: management; orbital; periorbital; treatment; venous malformation.
Figures




References
LinkOut - more resources
Full Text Sources
Other Literature Sources