

Prolonged survival in patients with breast cancer and a history of brain metastases: results of a preplanned subgroup analysis from the randomized phase III BEACON trial
- PMID: 28612225
- PMCID: PMC5543189
- DOI: 10.1007/s10549-017-4304-7
Prolonged survival in patients with breast cancer and a history of brain metastases: results of a preplanned subgroup analysis from the randomized phase III BEACON trial
Erratum in
-
Erratum to: Prolonged survival in patients with breast cancer and a history of brain metastases: results of a preplanned subgroup analysis from the randomized phase III BEACON trial.Breast Cancer Res Treat. 2017 Nov;166(1):327-328. doi: 10.1007/s10549-017-4482-3. Breast Cancer Res Treat. 2017. PMID: 28884461 Free PMC article. No abstract available.
Abstract
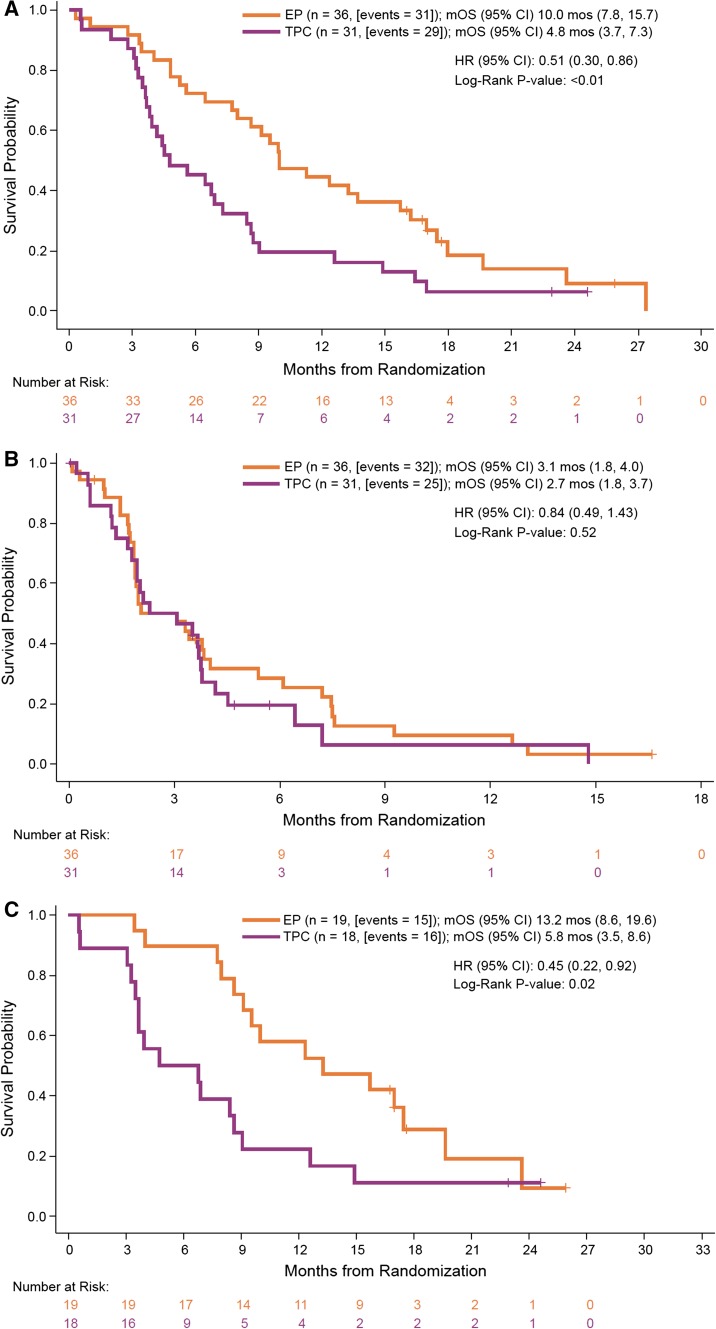
Purpose: Conventional chemotherapy has limited activity in patients with breast cancer and brain metastases (BCBM). Etirinotecan pegol (EP), a novel long-acting topoisomerase-1 inhibitor, was designed using advanced polymer technology to preferentially accumulate in tumor tissue including brain metastases, providing sustained cytotoxic SN38 levels.
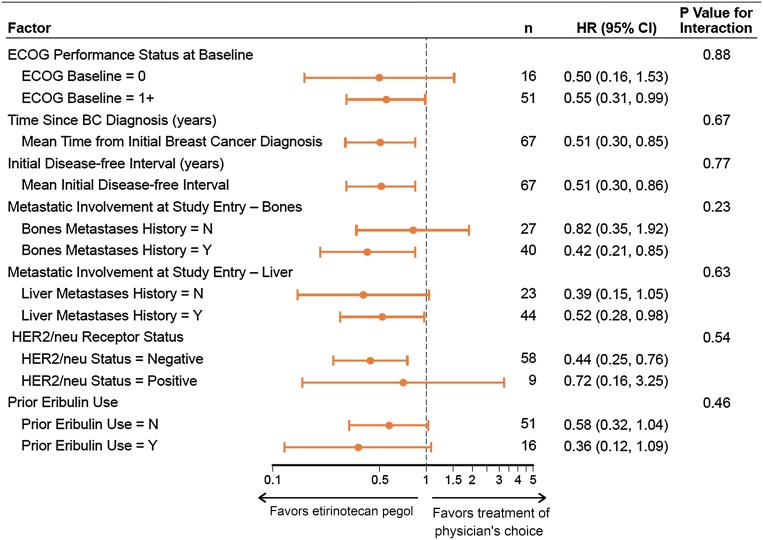
Methods: The phase 3 BEACON trial enrolled 852 women with heavily pretreated locally recurrent or metastatic breast cancer between 2011 and 2013. BEACON compared EP with treatment of physician's choice (TPC; eribulin, vinorelbine, gemcitabine, nab-paclitaxel, paclitaxel, ixabepilone, or docetaxel) in patients previously treated with anthracycline, taxane, and capecitabine, including those with treated, stable brain metastases. The primary endpoint, overall survival (OS), was assessed in a pre-defined subgroup of BCBM patients; an exploratory post hoc analysis adjusting for the diagnosis-specific graded prognostic assessment (GPA) index was also conducted.
Results: In the trial, 67 BCBM patients were randomized (EP, n = 36; TPC, n = 31). Treatment subgroups were balanced for baseline characteristics and GPA indices. EP was associated with a significant reduction in the risk of death (HR 0.51; P < 0.01) versus TPC; median OS was 10.0 and 4.8 months, respectively. Improvement in OS was observed in both poorer and better GPA prognostic groups. Survival rates at 12 months were 44.4% for EP versus 19.4% for TPC. Consistent with the overall BEACON population, fewer patients on EP experienced grade ≥3 toxicity (50 vs. 70%).
Conclusions: The significant improvement in survival in BCBM patients provides encouraging data for EP in this difficult-to-treat subgroup of patients. A phase three trial of EP in BCBM patients is underway (ClinicalTrials.gov NCT02915744).
Trial registration: ClinicalTrials.gov NCT01492101.
Keywords: Brain metastases; Chemotherapy; Etirinotecan pegol; Metastatic breast cancer; NKTR-102.
Conflict of interest statement
JC: advisor: Celgene, Roche; speaker: Celgene, Roche, Eisai, Novartis; partner and stockholder: MedSIR. HSR: research support to UC Regents from Eisai and from Nektar for this trial. AA: advisor: Nektar Therapeutics, Roche, Bayer, Pfizer. CJT: advisor: Nektar Therapeutics. VD: advisor: Roche, Novartis, Pfizer, Nektar, Eisai, Lilly; speaker: Roche, Pfizer, Novartis. CZ, MT, and UH: paid employees of Nektar Therapeutics. ALH: consultant, Nektar Therapeutics. JO: advisor: Nektar Therapeutics. EAP, S-AI, LSS, PG-P, DAY, DAP, AM, AM-A, and J-SA declare no conflicts of interest.
Figures
References
-
- Pestalozzi BC, Zahrieh D, Price KN, Holmberg SB, Lindtner J, Collins J, Crivellari D, Fey MF, Murray E, Pagani O, Simoncini E, Castiglione-Gertsch M, Gelber RD, Coates AS, Goldhirsch A; International Breast Cancer Study Group (IBCSG) Identifying breast cancer patients at risk for central nervous system (CNS) metastases in trials of the International Breast Cancer Study Group (IBCSG) Ann Oncol. 2006;17(6):935–944. doi: 10.1093/annonc/mdl064. - DOI - PubMed
-
- Lombardi G, Di Stefano AL, Farina P, Zagonel V, Tabouret E. Systemic treatments for brain metastases from breast cancer, non-small cell lung cancer, melanoma and renal cell carcinoma: an overview of the literature. Cancer Treat Rev. 2014;40(8):951–959. doi: 10.1016/j.ctrv.2014.05.007. - DOI - PubMed
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
