

High-Attenuation Areas on Chest Computed Tomography and Clinical Respiratory Outcomes in Community-Dwelling Adults
- PMID: 28613921
- PMCID: PMC5736977
- DOI: 10.1164/rccm.201703-0555OC
High-Attenuation Areas on Chest Computed Tomography and Clinical Respiratory Outcomes in Community-Dwelling Adults
Abstract
Rationale: Areas of increased lung attenuation visualized by computed tomography are associated with all-cause mortality in the general population. It is uncertain whether this association is attributable to interstitial lung disease (ILD).
Objectives: To determine whether high-attenuation areas are associated with the risk of ILD hospitalization and mortality in the general population.
Methods: We performed a cohort study of 6,808 adults aged 45-84 years sampled from six communities in the United States. High-attenuation areas were defined as the percentage of imaged lung volume with attenuation values between -600 and -250 Hounsfield units. An adjudication panel determined ILD hospitalization and death.
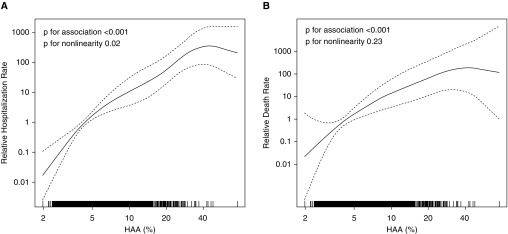
Measurements and main results: After adjudication, 52 participants had a diagnosis of ILD during 75,232 person-years (median, 12.2 yr) of follow-up. There were 48 hospitalizations attributable to ILD (crude rate, 6.4 per 10,000 person-years). Twenty participants died as a result of ILD (crude rate, 2.7 per 10,000 person-years). High-attenuation areas were associated with an increased rate of ILD hospitalization (adjusted hazard ratio, 2.6 per 1-SD increment in high-attenuation areas; 95% confidence interval, 1.9-3.5; P < 0.001), a finding that was stronger among men, African Americans, and Hispanics. High-attenuation areas were also associated with an increased rate of ILD-specific death (adjusted hazard ratio, 2.3; 95% confidence interval, 1.7-3.0; P < 0.001). Our findings were consistent among both smokers and nonsmokers.
Conclusions: Areas of increased lung attenuation are a novel risk factor for ILD hospitalization and mortality. Measurement of high-attenuation areas by screening and diagnostic computed tomography may be warranted in at-risk adults.
Keywords: epidemiology; hospitalizations; mortality; pulmonary fibrosis; subclinical interstitial lung disease.
Figures
Comment in
-
Toward Early Identification of Clinically Relevant Interstitial Lung Disease.Am J Respir Crit Care Med. 2017 Dec 1;196(11):1368-1369. doi: 10.1164/rccm.201706-1235ED. Am J Respir Crit Care Med. 2017. PMID: 28731358 Free PMC article. No abstract available.
References
-
- Raghu G, Chen SY, Yeh WS, Maroni B, Li Q, Lee YC, Collard HR. Idiopathic pulmonary fibrosis in US Medicare beneficiaries aged 65 years and older: incidence, prevalence, and survival, 2001–11. Lancet Respir Med. 2014;2:566–572. - PubMed
-
- Hutchinson JP, McKeever TM, Fogarty AW, Navaratnam V, Hubbard RB. Increasing global mortality from idiopathic pulmonary fibrosis in the twenty-first century. Ann Am Thorac Soc. 2014;11:1176–1185. - PubMed
-
- Christie JD, Edwards LB, Aurora P, Dobbels F, Kirk R, Rahmel AO, Taylor DO, Kucheryavaya AY, Hertz MI. Registry of the International Society for Heart and Lung Transplantation: twenty-fifth official adult lung and heart/lung transplantation report—2008. J Heart Lung Transplant. 2008;27:957–969. - PubMed
Publication types
MeSH terms
Grants and funding
- HHSN268201500003C/HL/NHLBI NIH HHS/United States
- N01 HC095161/HL/NHLBI NIH HHS/United States
- N01 HC095168/HL/NHLBI NIH HHS/United States
- T32 HL105323/HL/NHLBI NIH HHS/United States
- R01 HL077612/HL/NHLBI NIH HHS/United States
- N01 HC095159/HL/NHLBI NIH HHS/United States
- R01 HL093081/HL/NHLBI NIH HHS/United States
- N01 HC095163/HL/NHLBI NIH HHS/United States
- HHSN268201500003I/HL/NHLBI NIH HHS/United States
- P30 DK054759/DK/NIDDK NIH HHS/United States
- UL1 TR000040/TR/NCATS NIH HHS/United States
- N01 HC095166/HL/NHLBI NIH HHS/United States
- N01 HC095160/HL/NHLBI NIH HHS/United States
- UL1 TR001079/TR/NCATS NIH HHS/United States
- P30 ES005605/ES/NIEHS NIH HHS/United States
- R01 HL112986/HL/NHLBI NIH HHS/United States
- N01 HC095169/HL/NHLBI NIH HHS/United States
- N01 HC095167/HL/NHLBI NIH HHS/United States
- RC1 HL100543/HL/NHLBI NIH HHS/United States
- N01 HC095162/HL/NHLBI NIH HHS/United States
- K24 HL131937/HL/NHLBI NIH HHS/United States
- R01 HL103676/HL/NHLBI NIH HHS/United States
- N01 HC095165/HL/NHLBI NIH HHS/United States
- K24 HL103844/HL/NHLBI NIH HHS/United States
- N01 HC095164/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
