

Obstructive Sleep Apnea and Subclinical Interstitial Lung Disease in the Multi-Ethnic Study of Atherosclerosis (MESA)
- PMID: 28613935
- PMCID: PMC5711259
- DOI: 10.1513/AnnalsATS.201701-091OC
Obstructive Sleep Apnea and Subclinical Interstitial Lung Disease in the Multi-Ethnic Study of Atherosclerosis (MESA)
Abstract
Rationale: Obstructive sleep apnea (OSA) has been postulated to contribute to idiopathic pulmonary fibrosis by promoting alveolar epithelial injury via tractional forces and intermittent hypoxia.
Objectives: To determine whether OSA is associated with subclinical interstitial lung disease (ILD) and with biomarkers of alveolar epithelial injury and remodeling.
Methods: We performed cross-sectional analyses of 1,690 community-dwelling adults who underwent 15-channel in-home polysomnography and thoracic computed tomographic imaging in the Multi-Ethnic Study of Atherosclerosis. We measured the obstructive apnea-hypopnea index (oAHI) by polysomnography and high-attenuation areas (HAAs) and interstitial lung abnormalities (ILAs) by computed tomography. Serum matrix metalloproteinase-7 (MMP-7) and surfactant protein-A (SP-A) were measured by ELISA in 99 participants. We used generalized linear models to adjust for potential confounders.
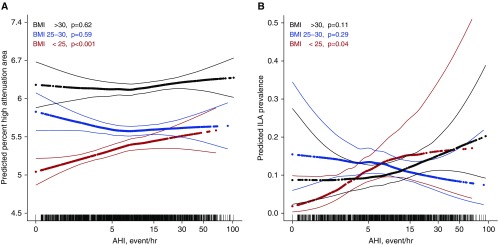
Results: The mean age was 68 years, and the mean forced vital capacity was 97% predicted. The median oAHI was 8.4 events/h, and 32% had an oAHI greater than 15. After adjusting for demographics, smoking, and center, an oAHI greater than 15 was associated with a 4.0% HAA increment (95% confidence interval [CI], 1.4-6.8%; P = 0.003) and 35% increased odds of ILA (95% CI, 13-61%; P = 0.001). However, there was evidence that these associations varied by body mass index (BMI) (P for interaction = 0.08 and 0.04, respectively). Among those with a BMI less than 25 kg/m2, an oAHI greater than 15 was associated with a 6.1% HAA increment (95% CI, 0.5-12%; P = 0.03) and 2.3-fold increased odds of ILA (95% CI, 1.3-4.1; P = 0.005). Among those with a BMI greater than 30 kg/m2, an oAHI greater than 15 was associated with 1.8-fold greater odds of ILA (95% CI, 1.1-2.9; P = 0.01) but was not associated with HAA. There were no meaningful associations detected among those with a BMI of 25-30 kg/m2. Greater oAHI was associated higher serum SP-A and MMP-7 levels, particularly among those with a BMI less than 25 kg/m2.
Conclusions: Moderate to severe OSA is associated with subclinical ILD and with evidence of alveolar epithelial injury and extracellular matrix remodeling in community-dwelling adults, an association that is strongest among normal-weight individuals. These findings support the hypothesis that OSA might contribute to early ILD.
Keywords: biomarkers; epidemiologic studies; interstitial lung disease; lung injury; sleep apnea.
Figures
Comment in
-
Can a Floppy Upper Airway Lead to Stiff Lungs?Ann Am Thorac Soc. 2017 Dec;14(12):1759-1760. doi: 10.1513/AnnalsATS.201707-519ED. Ann Am Thorac Soc. 2017. PMID: 29192817 No abstract available.
References
-
- King TE, Jr, Pardo A, Selman M. Idiopathic pulmonary fibrosis. Lancet. 2011;378:1949–1961. - PubMed
-
- Leslie KO. Idiopathic pulmonary fibrosis may be a disease of recurrent, tractional injury to the periphery of the aging lung: a unifying hypothesis regarding etiology and pathogenesis. Arch Pathol Lab Med. 2012;136:591–600. - PubMed
MeSH terms
Substances
Grants and funding
- HHSN268201500003C/HL/NHLBI NIH HHS/United States
- N01 HC095161/HL/NHLBI NIH HHS/United States
- N01 HC095168/HL/NHLBI NIH HHS/United States
- T32 HL105323/HL/NHLBI NIH HHS/United States
- R01 HL077612/HL/NHLBI NIH HHS/United States
- N01 HC095167/HL/NHLBI NIH HHS/United States
- N01 HC095159/HL/NHLBI NIH HHS/United States
- R01 HL093081/HL/NHLBI NIH HHS/United States
- R01 HL098433/HL/NHLBI NIH HHS/United States
- N01 HC095163/HL/NHLBI NIH HHS/United States
- HHSN268201500003I/HL/NHLBI NIH HHS/United States
- UL1 TR000040/TR/NCATS NIH HHS/United States
- N01 HC095166/HL/NHLBI NIH HHS/United States
- N01 HC095160/HL/NHLBI NIH HHS/United States
- UL1 TR001079/TR/NCATS NIH HHS/United States
- P30 ES005605/ES/NIEHS NIH HHS/United States
- R01 HL112986/HL/NHLBI NIH HHS/United States
- N01 HC095169/HL/NHLBI NIH HHS/United States
- N01 HC095162/HL/NHLBI NIH HHS/United States
- K24 HL131937/HL/NHLBI NIH HHS/United States
- R01 HL103676/HL/NHLBI NIH HHS/United States
- N01 HC095165/HL/NHLBI NIH HHS/United States
- K24 HL103844/HL/NHLBI NIH HHS/United States
- N01 HC095164/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
