

Third-line chemotherapy in advanced gastric cancer: A systematic review and meta-analysis
- PMID: 28614219
- PMCID: PMC5478304
- DOI: 10.1097/MD.0000000000006884
Third-line chemotherapy in advanced gastric cancer: A systematic review and meta-analysis
Abstract
Backgound: Little information regarding to the survival advantage of third-line chemotherapy in advanced gastric cancer patients is available. The current study is designed to systematically review and perform meta-analysis on the effect of third-line chemotherapy on progressive or recurrent gastric cancer treatment.
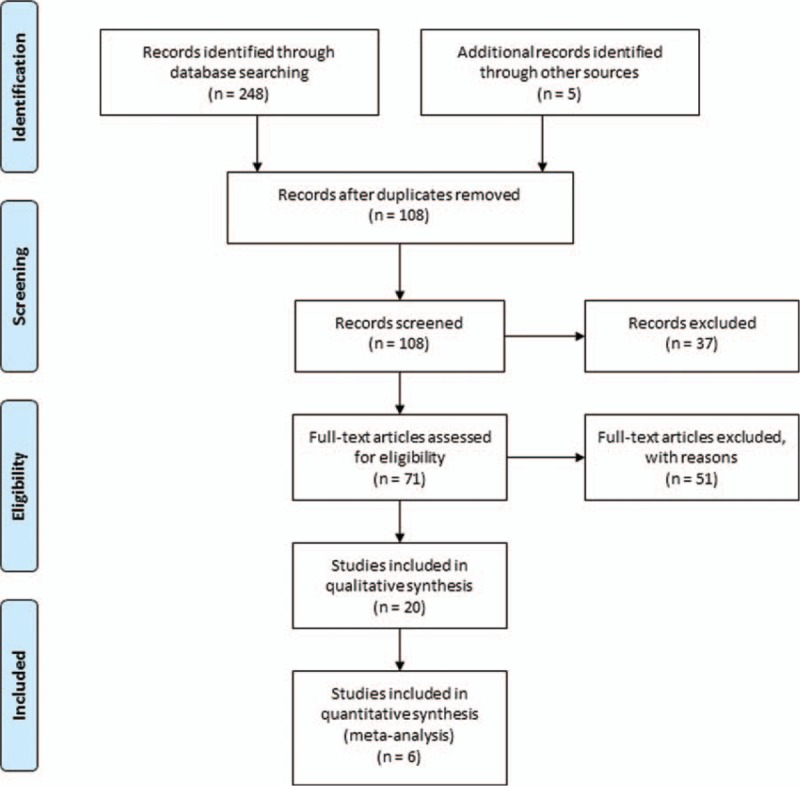
Methods: After thorough searching of online databases, total 20 articles were included into qualitative systematic review and 6 of them were used to conduct qualitative meta-analysis.
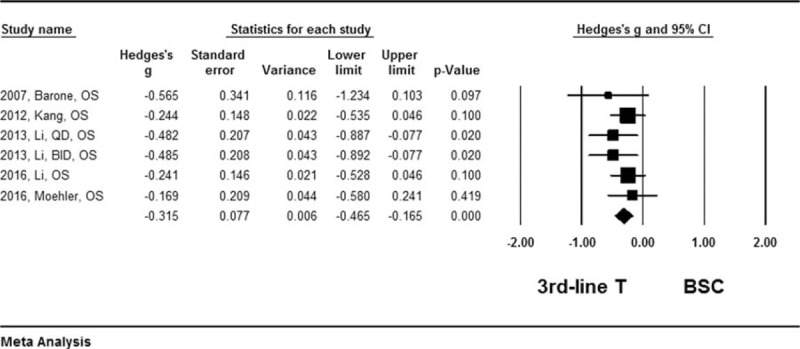
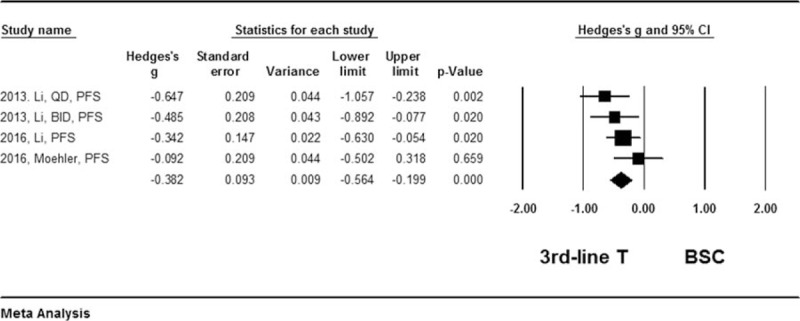
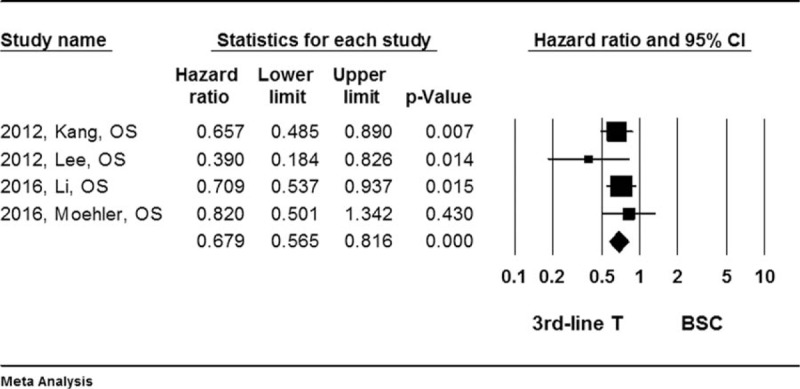
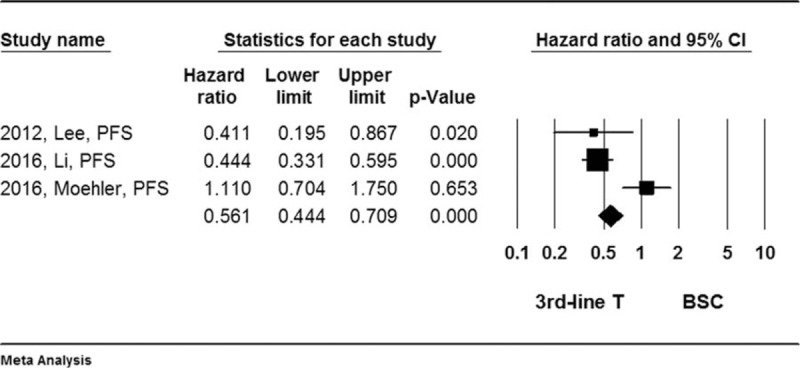
Results: It was found that the third-line chemotherapy was superior to placebo or best supportive care in terms of prolonging median oval survival (OS) length and progress free survival (PFS) length (Hedges's g for OS = -0.315 ± 0.077, P < .001; and for PFS = -0.382 ± 0.098, P < .001). In addition, the third-line chemotherapy was favored (Hedges's g = 0.848, P < .001) in terms of overall survival rate (Hazard ratio = 0.679, 95% confidence interval: 0.565-0.816, P < .001) or tumor free survival rate (Hazard ratio = 0.561, 95% confidence interval: 0.444-0.709, P < .001).
Conclusion: The third-line chemotherapy is superior to the best supportive care in advanced gastric cancer patients who had been pretreated with first-line and second-line chemotherapy.
Conflict of interest statement
The authors have no conflicts of interest to disclose.
Figures
References
-
- Siegel R, Ma J, Zou Z, et al. Cancer statistics, 2014. CA Cancer J Clin 2014;64:9–29. doi:10.3322/caac.21208. - PubMed
-
- Liu J, Sun L, Gong Y. Risk factors of precancerous gastric lesions in a population at high risk of gastric cancer. Chin J Cancer Res 2010;22:267–73.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
