

Pulmonary spindle cell carcinoma with unusual morphology: A rare case report and review of the literature
- PMID: 28614235
- PMCID: PMC5478320
- DOI: 10.1097/MD.0000000000007129
Pulmonary spindle cell carcinoma with unusual morphology: A rare case report and review of the literature
Abstract
Rationale: Pulmonary spindle cell carcinoma (PSCC) is a highly malignant carcinoma that often exhibits the histopathological characteristic of cell pleomorphism.
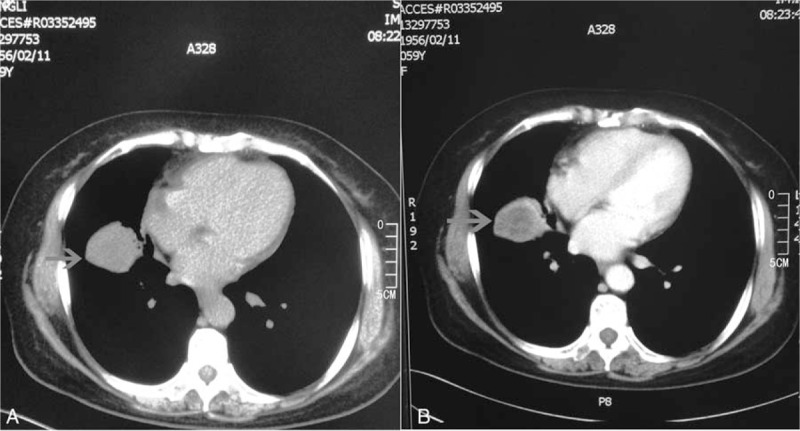
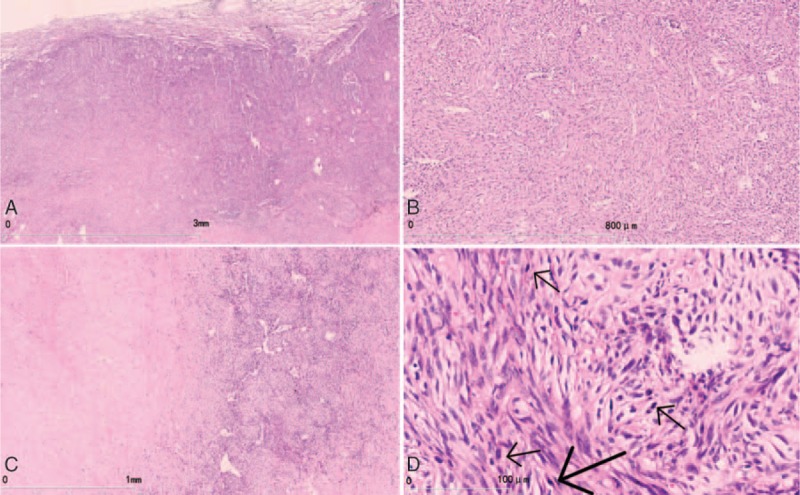
Patient concerns: Here, we report a PSCC case in a 59-year-old woman with multiple metastases. The pathological manifestation of this case did not show high-grade pleomorphism or atypia, and was easily mimicked by other borderline or low-grade malignant tumors such as an inflammatory myofibroblastic tumor (IMT).
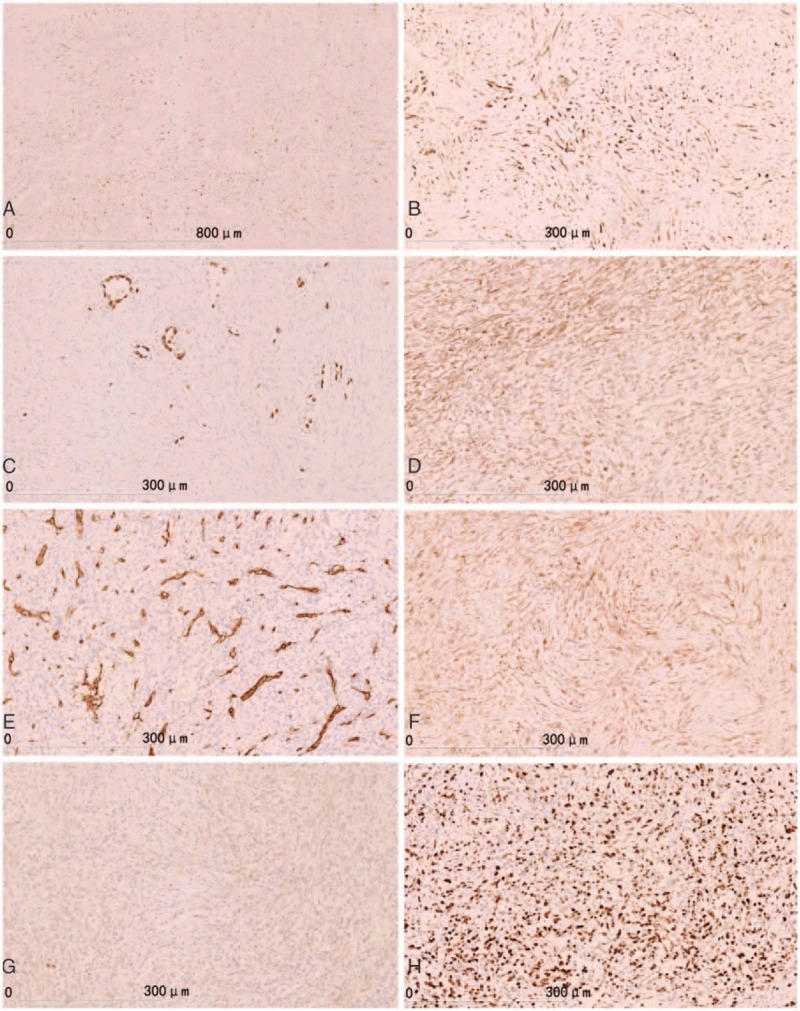
Diagnoses: Based on the results of immunohistochemistry and fluorescence in situ hybridization after the operation, IMT was ruled out, and PSCC was confirmed.
Interventions: Resection of the right middle lobe and dissection of the lymph nodes were performed. The patient was given 2 cycles of chemotherapy with cisplatin and 1 cycle of radiotherapy after the operation.
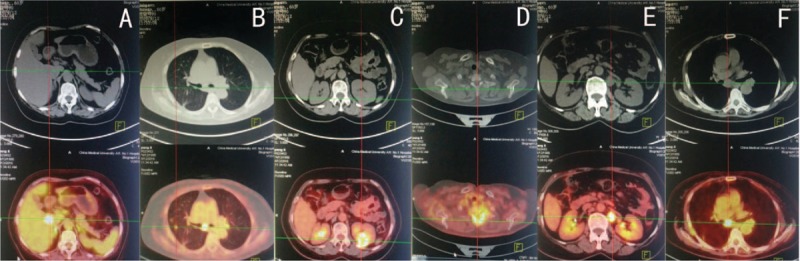
Outcomes: Metastatic lesions in the left kidney, the right lung, the first thoracic vertebrae, the retroperitoneal lymph nodes, and the mediastinal lymph nodes were identified by positron emission tomography/computed tomography 4 months after the operation, and the patient died 2 months later.
Lessons: PSCC is a highly malignant carcinoma, but it rarely shows a low-grade malignant histological morphology. So, efforts should be focused on differentiating it from other borderline or low malignant tumors (such as IMT) to avoid misdiagnosis.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Yun YL, Lee YC, Shih JY, et al. Pulmonary pleomorphic (spindle) cell carcinoma: peculiar clinicopathologic manifestations different from ordinary non-small cell carcinoma. Lung Cancer 2001;34:91–7. - PubMed
-
- Shigeta T, Minamikawa T, Matsui T, et al. Spindle cell carcinoma of the oral cavity: the impact of chemotherapy on pulmonary metastatic tumor doubling time. Kobe J Med Sci 2015;61:E64–70. - PubMed
-
- Travis WD, Brambilla E, Burke AP, et al. WHO Classification of Tumours of the Lung, Pleura, Thymus and Heart. 4th ed2015;Lyon: International Agency for Research on Cancer, 9-96. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
