

Thymectomy via open surgery or robotic video assisted thoracic surgery: Can a recommendation already be made?
- PMID: 28614249
- PMCID: PMC5478334
- DOI: 10.1097/MD.0000000000007161
Thymectomy via open surgery or robotic video assisted thoracic surgery: Can a recommendation already be made?
Abstract
Background: Robot-assisted minimally invasive surgery (RVATS) is a relatively new technique applied for thymectomies. Only few studies directly compare RVATS to the mainstay therapy, open surgery (sternotomy).
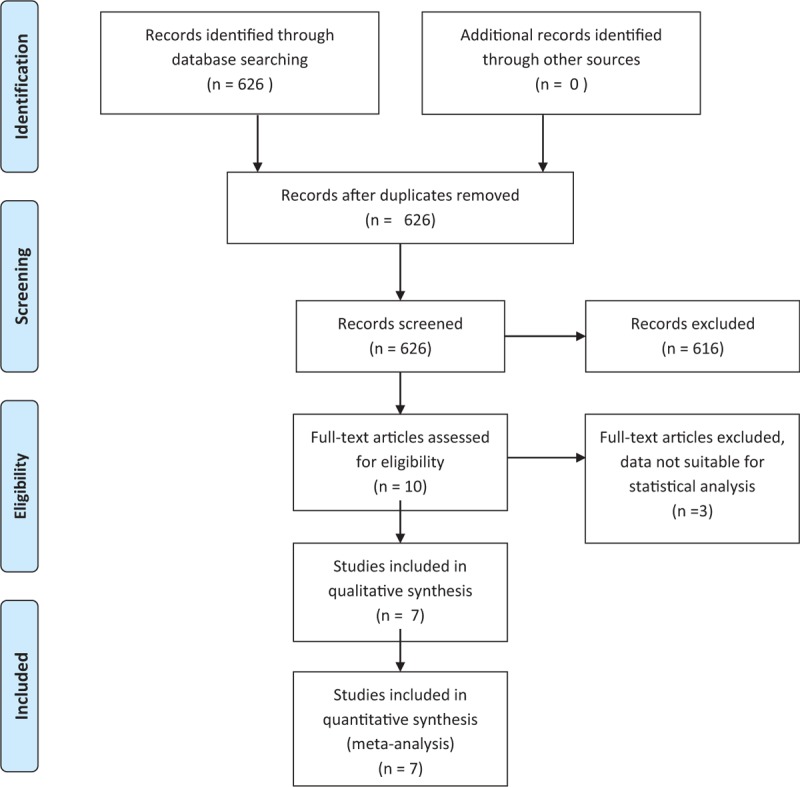
Methods: A systematic search of the literature was performed in October 2016. The meta-analysis includes studies comparing robotassisted and open thymectomy regarding operation time, length of hospitalization, intraoperative blood loss, and chest-in-tube days, postoperative complications, reoperation, arrhythmic events, pleural effusion, and postoperative bleeding.
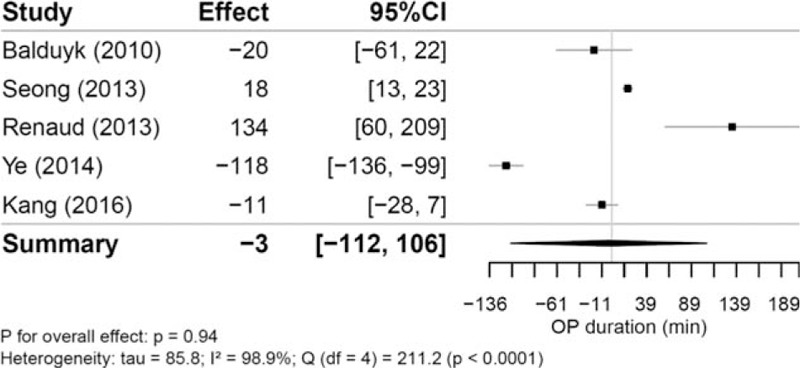
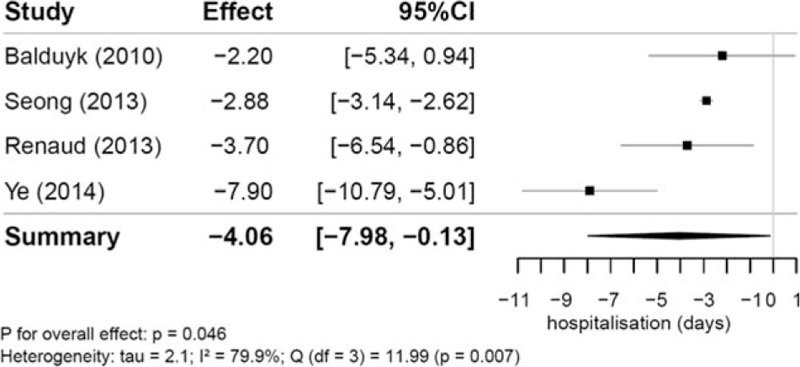
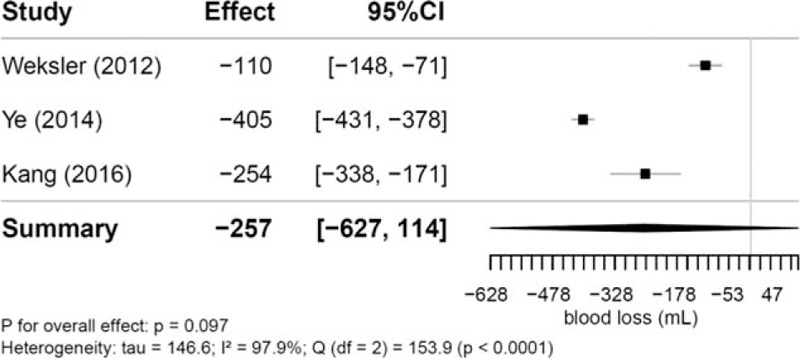
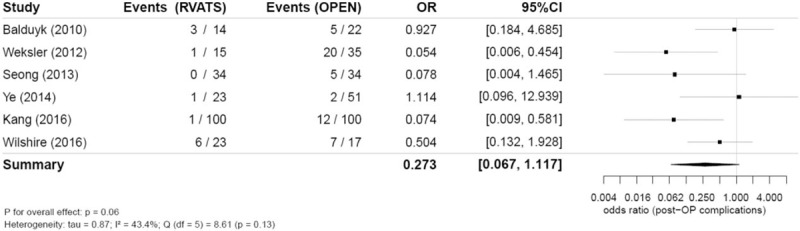
Results: Of 626 studies preliminary screened, 7 articles were included. There were no significant differences in comparison of operation time (-3.19 minutes [95% confidence interval, 95% CI -112.43 to 106.05]; P = .94), but patients undergoing RVATS spent significantly less time in hospital (-4.06 days [95% CI -7.98 to -0.13], P = .046). There were fewer chests-in-tube days (-2.50 days [95% CI -15.01 to 10.01]; P = .24) and less intraoperative blood loss (-256.84 mL [95% CI -627.47 to 113.80]; P = .10) observed in the RVATS group; due to a small number of studies, these results were not statistically significant. There were also less post-operative complications in the RVATS group (12 complications in 209 patients vs 51 complications in 259 patients); however, this difference was not statistical significant (odds ratio 0.27, 95% CI 0.07-1.12; P = .06).
Conclusions: Patients undergoing RVATS spent less time in hospital than patients treated by open surgery (sternotomy). These patients tended to have less postoperative complications, less intraoperative blood loss, and fewer chest-in-tube days. We found evidence for the safety and feasibility of RVATS compared with open surgery, which has to be further confirmed in randomised controlled trials.
Conflict of interest statement
The authors have no conflict of interest.
Figures
Similar articles
-
Perioperative Outcomes of Thymectomy in Myasthenia Gravis: A Thoracic Surgery Database Analysis.Ann Thorac Surg. 2022 Mar;113(3):904-910. doi: 10.1016/j.athoracsur.2021.06.071. Epub 2021 Jul 30. Ann Thorac Surg. 2022. PMID: 34339670
-
Robotic versus thoracoscopic thymectomy: The current evidence.Int J Med Robot. 2017 Dec;13(4). doi: 10.1002/rcs.1847. Epub 2017 Jun 29. Int J Med Robot. 2017. PMID: 28660682 Review.
-
Comparative study for surgical management of thymectomy for non-thymomatous myasthenia gravis from the French national database EPITHOR.Eur J Cardiothorac Surg. 2016 Sep;50(3):418-22. doi: 10.1093/ejcts/ezw064. Epub 2016 Mar 16. Eur J Cardiothorac Surg. 2016. PMID: 26984980
-
[Thymomectomy by minimally invasive surgery. Comparative study videosurgery versus robot-assisted surgery].Rev Mal Respir. 2017 May;34(5):544-552. doi: 10.1016/j.rmr.2017.01.002. Epub 2017 Feb 16. Rev Mal Respir. 2017. PMID: 28216170 French.
-
Robot-assisted thoracic surgery versus video-assisted thoracic surgery for treatment of patients with thymoma: A systematic review and meta-analysis.Thorac Cancer. 2022 Jan;13(2):151-161. doi: 10.1111/1759-7714.14234. Epub 2021 Nov 22. Thorac Cancer. 2022. PMID: 34806328 Free PMC article.
Cited by
-
Relevance of robotic surgery for thymoma: a narrative review.Mediastinum. 2024 May 21;8:29. doi: 10.21037/med-23-37. eCollection 2024. Mediastinum. 2024. PMID: 38881811 Free PMC article. Review.
-
Complications of robot-assisted thymectomy: A single-arm meta-analysis and systematic review.Int J Med Robot. 2021 Dec;17(6):e2333. doi: 10.1002/rcs.2333. Epub 2021 Sep 24. Int J Med Robot. 2021. PMID: 34533876 Free PMC article.
-
Pediatric thymectomy: a study of national trends in demographics, short-term outcomes, and cost.Pediatr Surg Int. 2019 Jul;35(7):749-757. doi: 10.1007/s00383-019-04486-1. Epub 2019 May 22. Pediatr Surg Int. 2019. PMID: 31119357
-
Optimal management of thymic malignancies: current perspectives.Cancer Manag Res. 2019 Jul 22;11:6803-6814. doi: 10.2147/CMAR.S171683. eCollection 2019. Cancer Manag Res. 2019. PMID: 31413632 Free PMC article.
-
Robot-assisted thoracic surgery in Colombia: a multi-institutional initial experience.Ann Cardiothorac Surg. 2019 Mar;8(2):233-240. doi: 10.21037/acs.2019.03.01. Ann Cardiothorac Surg. 2019. PMID: 31032207 Free PMC article.
References
-
- Girard N, Mornex F, Houtte PV, et al. Thymoma: a focus on current therapeutic management. J Thorac Oncol 2009;4:119–26. - PubMed
-
- Masaoka A, Monden Y, Nakahara K, et al. Follow-up study of thymomas with special reference to their clinical stages. Cancer 1981;48:2485–92. - PubMed
-
- Scorsetti M, Leo F, Trama A, et al. Thymoma and thymic carcinomas. Crit Rev Oncol Hematol 2016;99:332–50. - PubMed
-
- Ashton RC, Connery CP, Swistel DG, et al. Robot-assisted lobectomy. J Thorac Cardiovasc Surg 2003;126:292–3. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
