

Clinical, Biochemical, and Genetic Characterization of North American Patients With Erythropoietic Protoporphyria and X-linked Protoporphyria
- PMID: 28614581
- PMCID: PMC5710403
- DOI: 10.1001/jamadermatol.2017.1557
Clinical, Biochemical, and Genetic Characterization of North American Patients With Erythropoietic Protoporphyria and X-linked Protoporphyria
Abstract
Importance: Autosomal recessive erythropoietic protoporphyria (EPP) and X-linked protoporphyria (XLP) are rare photodermatoses presenting with variable degrees of painful phototoxicity that markedly affects quality of life. The clinical variability, determinants of severity, and genotype/phenotype correlations of these diseases are not well characterized.
Objective: To describe the baseline clinical characteristics, genotypes, and determinants of disease severity in a large patient cohort with EPP or XLP.
Design, setting, and participants: A prospective observational study was conducted among patients with confirmed diagnoses of EPP or XLP from November 1, 2010, to December 6, 2015, at 6 academic medical centers of the Porphyrias Consortium of the National Institutes of Health Rare Diseases Clinical Research Network. Detailed medical histories, including history of phototoxicity and treatment, were collected on standardized case report forms. Patients underwent baseline laboratory testing, total erythrocyte protoporphyrin (ePPIX) testing, and molecular genetic testing. Data were entered into a centralized database.
Main outcomes and measures: Results of biochemical and genetic tests were explored for association with clinical phenotype in patients with EPP or XLP.
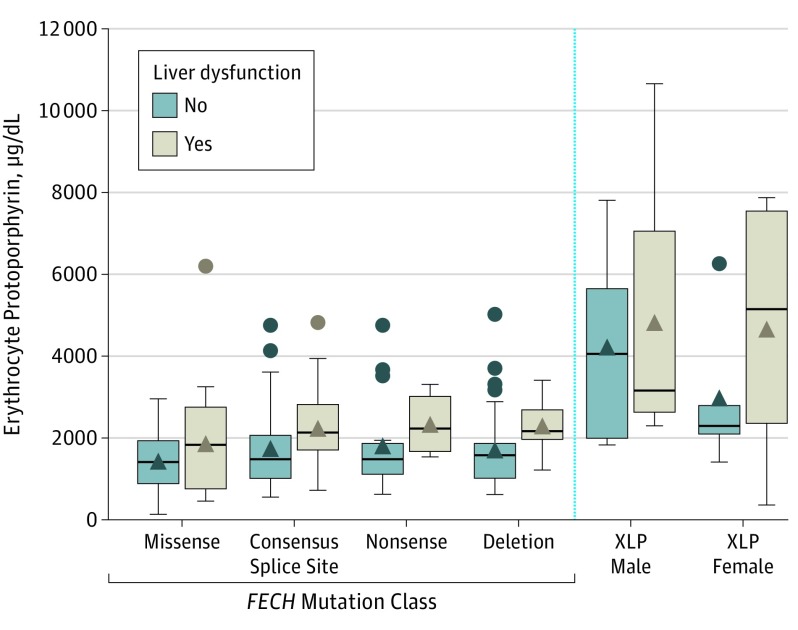
Results: Of the 226 patients in the study (113 female and 113 male patients; mean [SD] age, 36.7 [17.0] years), 186 (82.3%) had EPP with a FECH (OMIM 612386) mutation and the common low-expression FECH allele IVS3-48T>C, and only 1 patient had 2 FECH mutations. Twenty-two patients had XLP (9.7%; 10 male and 12 female patients), and 9 patients (4.0%) had elevated ePPIX levels and symptoms consistent with protoporphyria but no detectable mutation in the FECH or ALAS2 (OMIM 301300) gene. Samples of DNA could not be obtained from 8 patients. Patients' mean (SD) age at symptom onset was 4.4 (4.4) years. Anemia (107 [47.3%]), history of liver dysfunction (62 [27.4%]), and gallstones (53 [23.5%]) were commonly reported. Higher ePPIX levels were associated with earlier age of symptom onset (median ePPIX levels for those who developed symptoms before vs after 1 year of age, 1744 vs 1567 µg/dL; P = .02), less sun tolerance (median ePPIX levels for those reporting symptoms before vs after 10 minutes of sun exposure, 2233 vs 1524 µg/dL; P ≤ .001), and increased risk of liver dysfunction (median ePPIX levels for those with liver dysfunction vs normal liver function, 2016 vs 1510 µg/dL; P = .003). Patients with EPP and FECH missense mutations had significantly lower ePPIX levels than those with other mutations (1462 vs 1702 µg/dL; P = .01). Male patients with XLP had significantly higher ePPIX levels, on average, than did patients with EPP (3574 vs 1669 µg/dL; P < .001). Marked clinical variability was seen in female patients with XLP owing to random X-chromosomal inactivation.
Conclusions and relevance: These data suggest that higher ePPIX levels are a major determinant of disease severity and risk of liver dysfunction in patients with EPP or XLP. These findings provide a framework for clinical monitoring and management of these disorders.
Conflict of interest statement
Figures
References
-
- Anderson KE, Sassa S, Bishop DF, Desnick RJ. Disorders of heme biosynthesis: X-linked sideroblastic anemia and the porphyrias In: Scriver CR, Beadet AL, Sly WS, Valle D, eds. The Metabolic and Molecular Bases of Inherited Disease. Vol 2 8th ed New York: McGraw Hill; 2001:2991-3062.
-
- Bonkovsky HL, Guo JT, Hou W, Li T, Narang T, Thapar M. Porphyrin and heme metabolism and the porphyrias. Compr Physiol. 2013;3(1):365-401. - PubMed
-
- Poh-Fitzpatrick MB. Porphyrias: photosensitivity and phototherapy. Methods Enzymol. 2000;319:485-493. - PubMed
-
- Holme SA, Anstey AV, Finlay AY, Elder GH, Badminton MN. Erythropoietic protoporphyria in the UK: clinical features and effect on quality of life. Br J Dermatol. 2006;155(3):574-581. - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
