

Severe Pneumococcal Pneumonia Causes Acute Cardiac Toxicity and Subsequent Cardiac Remodeling
- PMID: 28614669
- PMCID: PMC5620668
- DOI: 10.1164/rccm.201701-0104OC
Severe Pneumococcal Pneumonia Causes Acute Cardiac Toxicity and Subsequent Cardiac Remodeling
Abstract
Rationale: Up to one-third of patients hospitalized with pneumococcal pneumonia experience major adverse cardiac events (MACE) during or after pneumonia. In mice, Streptococcus pneumoniae can invade the myocardium, induce cardiomyocyte death, and disrupt cardiac function following bacteremia, but it is unknown whether the same occurs in humans with severe pneumonia.
Objectives: We sought to determine whether S. pneumoniae can (1) translocate the heart, (2) induce cardiomyocyte death, (3) cause MACE, and (4) induce cardiac scar formation after antibiotic treatment during severe pneumonia using a nonhuman primate (NHP) model.
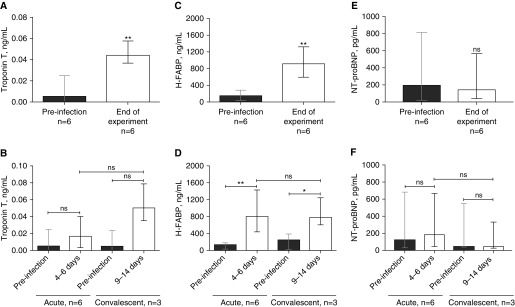
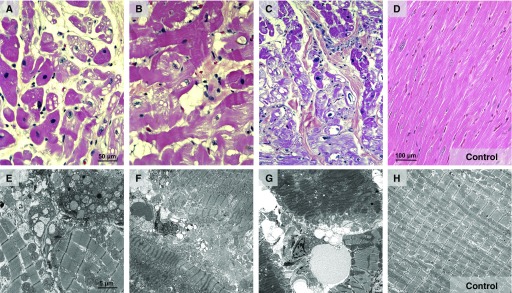
Methods: We examined cardiac tissue from six adult NHPs with severe pneumococcal pneumonia and three uninfected control animals. Three animals were rescued with antibiotics (convalescent animals). Electrocardiographic, echocardiographic, and serum biomarkers of cardiac damage were measured (troponin T, N-terminal pro-brain natriuretic peptide, and heart-type fatty acid binding protein). Histological examination included hematoxylin and eosin staining, immunofluorescence, immunohistochemistry, picrosirius red staining, and transmission electron microscopy. Immunoblots were used to assess the underlying mechanisms.
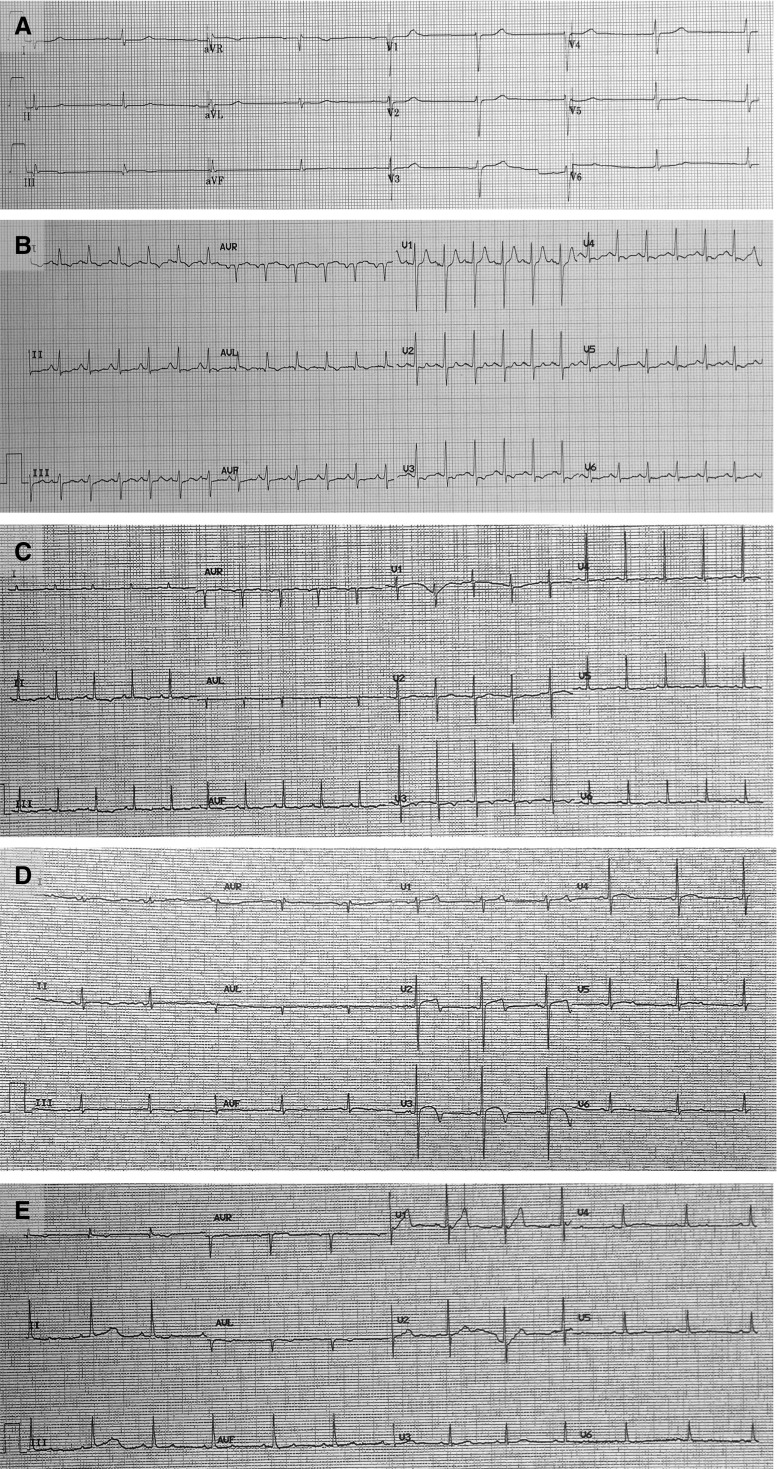
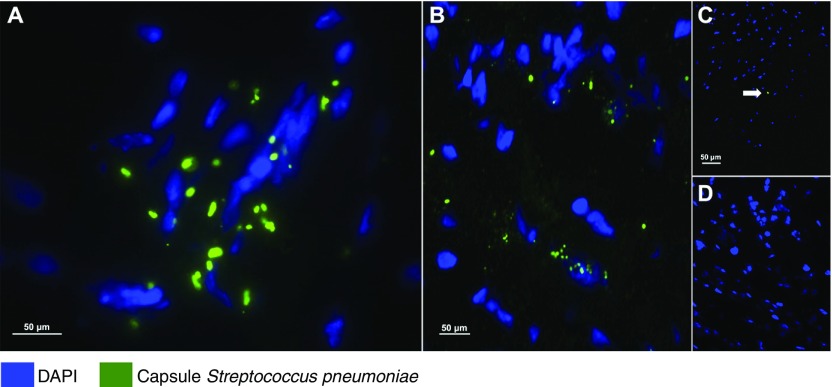
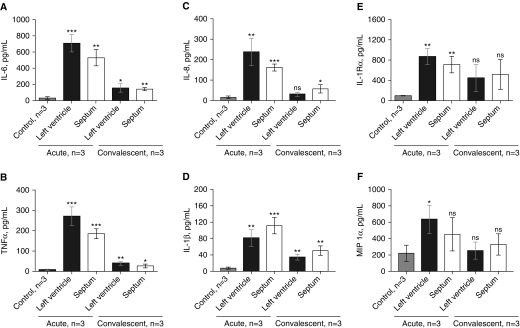
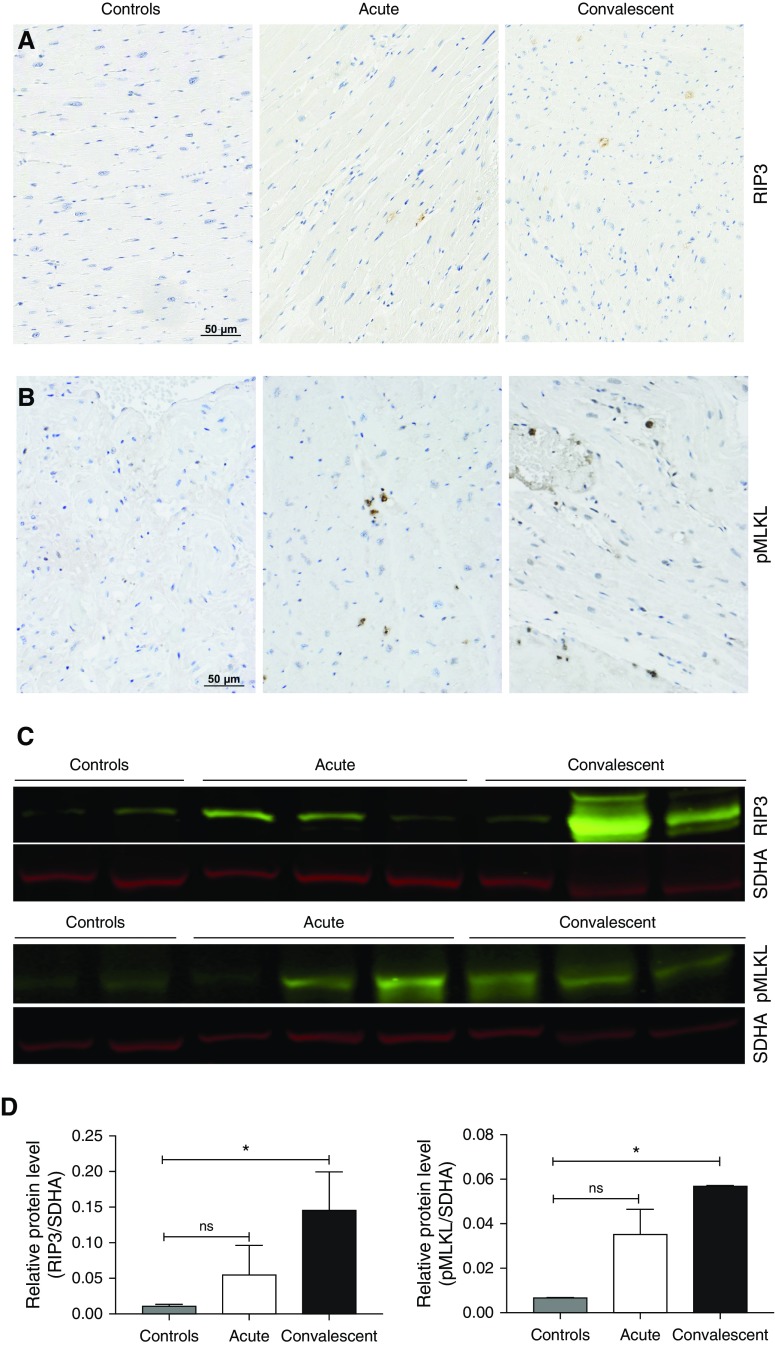
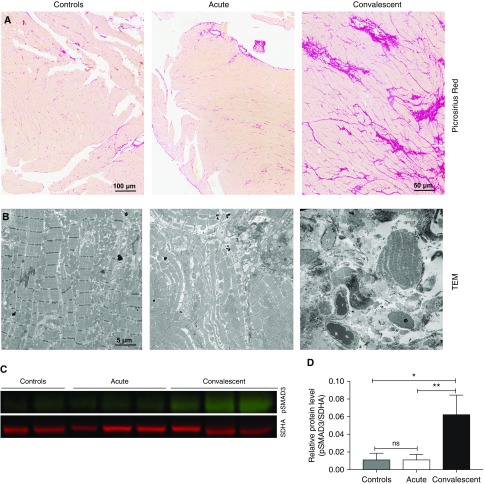
Measurements and main results: Nonspecific ischemic alterations were detected by electrocardiography and echocardiography. Serum levels of troponin T and heart-type fatty acid binding protein were increased (P < 0.05) after pneumococcal infection in both acutely ill and convalescent NHPs. S. pneumoniae was detected in the myocardium of all NHPs with acute severe pneumonia. Necroptosis and apoptosis were detected in the myocardium of both acutely ill and convalescent NHPs. Evidence of cardiac scar formation was observed only in convalescent animals by transmission electron microscopy and picrosirius red staining.
Conclusions: S. pneumoniae invades the myocardium and induces cardiac injury with necroptosis and apoptosis, followed by cardiac scarring after antibiotic therapy, in an NHP model of severe pneumonia.
Keywords: Streptococcus pneumoniae; cardiovascular complications; community-acquired pneumonia; pneumococcal pneumonia.
Figures
Comment in
-
Pneumonia and the Risk of Cardiovascular Death. Time to Change Our Strategy.Am J Respir Crit Care Med. 2017 Sep 1;196(5):541-543. doi: 10.1164/rccm.201707-1421ED. Am J Respir Crit Care Med. 2017. PMID: 28723315 No abstract available.
References
-
- Wunderink RG, Waterer GW. Community-acquired pneumonia. N Engl J Med. 2014;370:1863. - PubMed
-
- Torres A, Sibila O, Ferrer M, Polverino E, Menendez R, Mensa J, Gabarrús A, Sellarés J, Restrepo MI, Anzueto A, et al. Effect of corticosteroids on treatment failure among hospitalized patients with severe community-acquired pneumonia and high inflammatory response: a randomized clinical trial. JAMA. 2015;313:677–686. - PubMed
-
- Musher DM, Thorner AR. Community-acquired pneumonia. N Engl J Med. 2014;371:1619–1628. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
