

Development and validation of a risk score to assist screening for acute HIV-1 infection among men who have sex with men
- PMID: 28615005
- PMCID: PMC5471739
- DOI: 10.1186/s12879-017-2508-4
Development and validation of a risk score to assist screening for acute HIV-1 infection among men who have sex with men
Erratum in
-
Correction to: Development and validation of a risk score to assist screening for acute HIV-1 infection among men who have sex with men.BMC Infect Dis. 2017 Oct 24;17(1):691. doi: 10.1186/s12879-017-2805-y. BMC Infect Dis. 2017. PMID: 29065854 Free PMC article. No abstract available.
Abstract
Background: Early treatment of acute HIV-1 infection (AHI) is beneficial for patients and could reduce onward transmission. However, guidelines on whom to test for AHI with HIV-1 RNA testing are lacking.
Methods: A risk score for possible AHI based on literature and expert opinion - including symptoms associated with AHI and early HIV-1 - was evaluated using data from the Amsterdam Cohort Studies among men who have sex with men (MSM). Subsequently, we optimized the risk score by constructing two multivariable logistic regression models: one including only symptoms and one combining symptoms with known risk factors for HIV-1 seroconversion, using generalized estimating equations. Several risk scores were generated from these models and the optimal risk score was validated using data from the Multicenter AIDS Cohort Study.
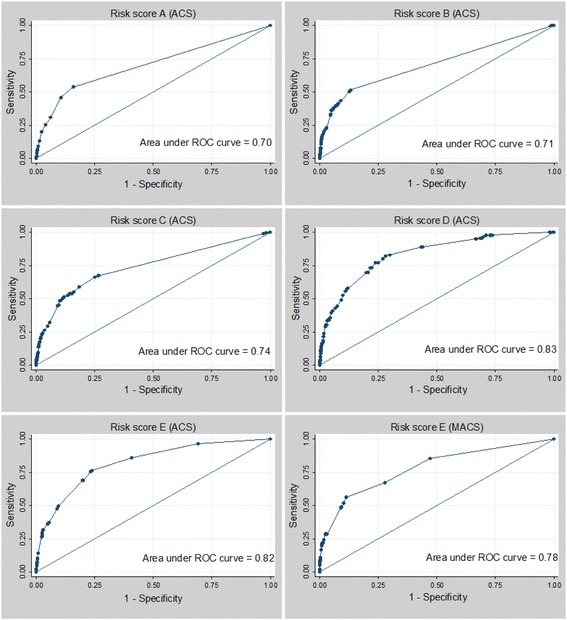
Results: Using data from 1562 MSM with 175 HIV-1 seroconversion visits and 17,271 seronegative visits in the Amsterdam Cohort Studies, the optimal risk score included four symptoms (oral thrush, fever, lymphadenopathy, weight loss) and three risk factors (self-reported gonorrhea, receptive condomless anal intercourse, more than five sexual partners, all in the preceding six months) and yielded an AUC of 0.82. Sensitivity was 76.3% and specificity 76.3%. Validation in the Multicenter AIDS Cohort Study resulted in an AUC of 0.78, sensitivity of 56.2% and specificity of 88.8%.
Conclusions: The optimal risk score had good overall performance in the Amsterdam Cohort Studies and performed comparable (but showed lower sensitivity) in the validation study. Screening for AHI with four symptoms and three risk factors would increase the efficiency of AHI testing and potentially enhance early diagnosis and immediate treatment.
Keywords: Acute HIV-1 infection; Diagnosis; MSM; Risk score; Screening tool.
Figures
References
-
- Panel on antiretroviral guidelines for adults and adolescents. Guidelines for the use of antiretroviral agents in HIV-1-infected adults and adolescents. Department of Health and Human Services. 2014. http://aidsinfo.Nih.Gov/ContentFiles/AdultandAdolescentGL.Pdf. Accessed 17 December 2016.
-
- Grijsen ML, Steingrover R, Wit FW, Jurriaans S, Verbon A, Brinkman K, van der Ende ME, Soetekouw R, de Wolf F, Lange JM, et al. No treatment versus 24 or 60 weeks of antiretroviral treatment during primary HIV infection: the randomized Primo-SHM trial. PLoS Med. 2012;9(3):e1001196. doi: 10.1371/journal.pmed.1001196. - DOI - PMC - PubMed
-
- Oxenius A, Price D, Easterbrook P, O’Callaghan C, Kelleher A, Whelan J, Sontag G, Sewell A, Phillips R. Early highly active antiretroviral therapy for acute HIV-1 infection preserves immune function of CD81 and CD41 T lymphocytes. PNAS. 2000;97(7):33823387. doi: 10.1073/pnas.97.7.3382. - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
