

Postoperative goal-directed therapy and development of acute kidney injury following major elective noncardiac surgery: post-hoc analysis of POM-O randomized controlled trial
- PMID: 28616213
- PMCID: PMC5466093
- DOI: 10.1093/ckj/sfw118
Postoperative goal-directed therapy and development of acute kidney injury following major elective noncardiac surgery: post-hoc analysis of POM-O randomized controlled trial
Abstract
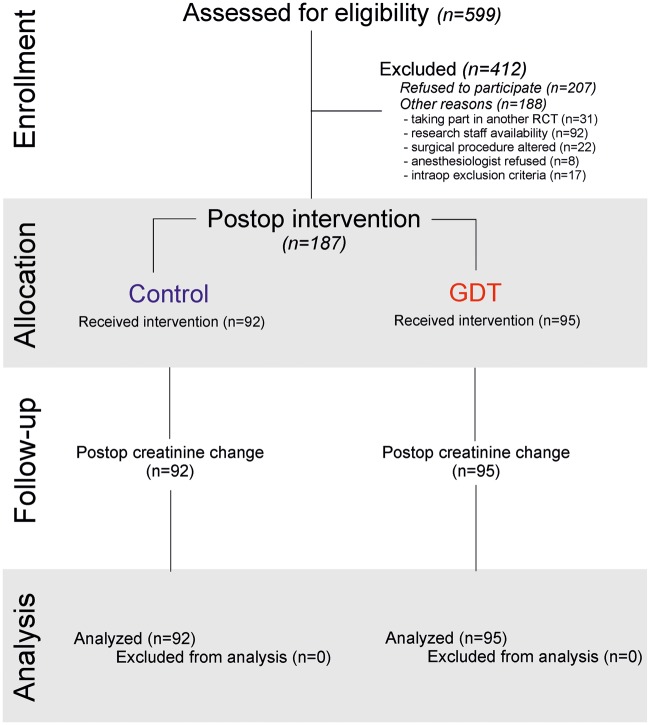
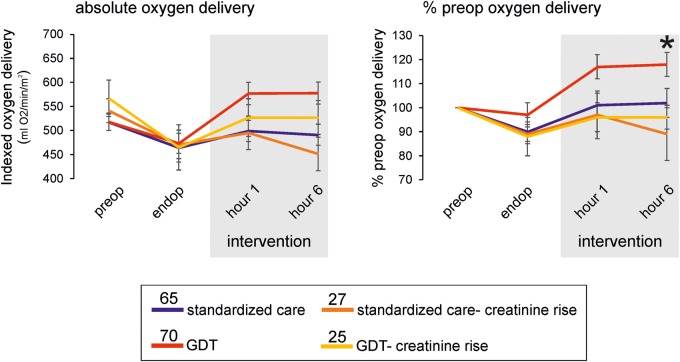
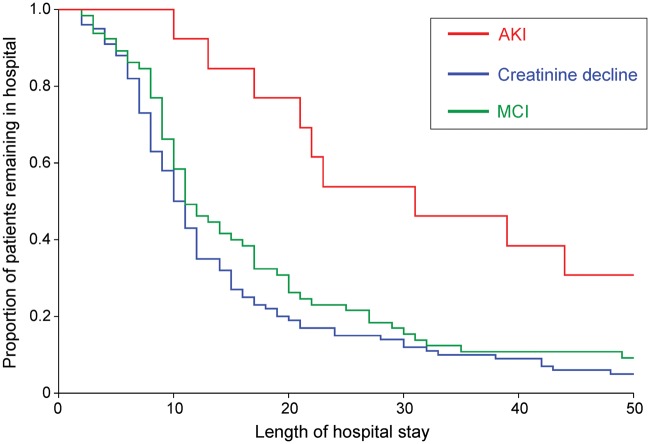
Background: The role of goal-directed therapy (GDT) in preventing creatinine rise following noncardiac surgery is unclear. We performed a post-hoc analysis of a randomized controlled trial to assess the relationship between postoperative optimization of oxygen delivery and development of acute kidney injury (AKI)/creatinine rise following noncardiac surgery. Methods: Patients were randomly assigned immediately postoperatively to receive either fluid and/or dobutamine therapy to maintain/restore their preoperative oxygen delivery, or protocolized standard care (oxygen delivery only recorded). Primary end point was serial changes in postoperative creatinine within 48 h postoperatively. Secondary outcomes were development of AKI (KDIGO criteria) and minimal creatinine rise (MCR; no decline from preoperative creatinine), related to all-cause morbidity and length of stay. Results: Postoperative reductions in serum creatinine were similar (P = 0.76) in patients randomized to GDT [10 µmol/L (95% confidence interval, CI: 17 to -1); n = 95] or protocolized care [8 µmol/L (95% CI: 17 to -6); n = 92]. Postoperative haemodynamic management was not associated with the development of MCR [78/187 (41.7%)] or AKI [13/187; (7.0%)]. Intraoperative requirement for norepinephrine was more likely in patients who developed postoperative rises in creatinine [relative risk (RR): 1.66 (95% CI: 1.04-2.67); P = 0.04], despite similar volumes of intraoperative fluid being administered. Persistently higher lactate during the intervention period was associated with AKI (mean difference: 1.15 mmol/L (95% CI: 0.48-1.81); P = 0.01]. Prolonged hospital stay was associated with AKI but not MCR [RR: 2.71 (95% CI: 1.51-4.87); P = 0.0008]. Conclusion: These data provide further insights into how perioperative haemodynamic alterations relate to postoperative increases in creatinine once systemic inflammation is established.
Keywords: acute kidney injury; cardiac output; noncardiac surgery; oxygen delivery.
Figures
Similar articles
-
Risk Stratification for Postoperative Acute Kidney Injury in Major Noncardiac Surgery Using Preoperative and Intraoperative Data.JAMA Netw Open. 2019 Dec 2;2(12):e1916921. doi: 10.1001/jamanetworkopen.2019.16921. JAMA Netw Open. 2019. PMID: 31808922 Free PMC article.
-
Acute kidney injury after lung resection surgery: incidence and perioperative risk factors.Anesth Analg. 2012 Jun;114(6):1256-62. doi: 10.1213/ANE.0b013e31824e2d20. Epub 2012 Mar 26. Anesth Analg. 2012. PMID: 22451594
-
Is Preoperative Endothelial Dysfunction a Potentially Modifiable Risk Factor for Renal Injury Associated With Noncardiac Surgery?J Cardiothorac Vasc Anesth. 2015 Oct;29(5):1220-8. doi: 10.1053/j.jvca.2015.05.116. Epub 2015 May 14. J Cardiothorac Vasc Anesth. 2015. PMID: 26384628
-
Intraoperative hypotension is associated with acute kidney injury in noncardiac surgery: An observational study.Eur J Anaesthesiol. 2018 Apr;35(4):273-279. doi: 10.1097/EJA.0000000000000735. Eur J Anaesthesiol. 2018. PMID: 29210843
-
Association Between Intraoperative Oliguria and Acute Kidney Injury After Major Noncardiac Surgery.Anesth Analg. 2018 Nov;127(5):1229-1235. doi: 10.1213/ANE.0000000000003576. Anesth Analg. 2018. PMID: 29933276
Cited by
-
The Effect of Intraoperative Hypotension on Postoperative Renal Function.Curr Anesthesiol Rep. 2023 Sep;13(3):181-186. doi: 10.1007/s40140-023-00564-2. Epub 2023 Jun 14. Curr Anesthesiol Rep. 2023. PMID: 39802614 Free PMC article.
-
Impact of Enhanced Recovery After Surgery (ERAS) protocol versus standard of care on postoperative Acute Kidney Injury (AKI): A meta-analysis.PLoS One. 2021 May 20;16(5):e0251476. doi: 10.1371/journal.pone.0251476. eCollection 2021. PLoS One. 2021. PMID: 34015002 Free PMC article.
-
Perioperative Renoprotection: General Mechanisms and Treatment Approaches.Anesth Analg. 2020 Dec;131(6):1679-1692. doi: 10.1213/ANE.0000000000005107. Anesth Analg. 2020. PMID: 33186157 Free PMC article. Review.
-
Hemodynamic goal-directed therapy and postoperative kidney injury: an updated meta-analysis with trial sequential analysis.Crit Care. 2019 Jun 26;23(1):232. doi: 10.1186/s13054-019-2516-4. Crit Care. 2019. PMID: 31242941 Free PMC article.
References
-
- Hoste EA, Bagshaw SM, Bellomo R. et al. Epidemiology of acute kidney injury in critically ill patients: the multinational AKI–EPI study. Intensive Care Med 2015; 41: 1411–1423 - PubMed
-
- O’Connor ME, Kirwan CJ, Pearse RM. et al. Incidence and associations of acute kidney injury after major abdominal surgery. Intensive Care Med 2016; 24: 521–530 - PubMed
-
- Bihorac A, Yavas S, Subbiah S. et al. Long-term risk of mortality and acute kidney injury during hospitalization after major surgery. Ann Surg 2009; 249: 851–858 - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
